Atraumatic Red Eye
Warning
Objectives
To guide the assessment and management of patients suffering from acute red eye including:
- Conjunctivitis
- Keratitis
- Uveitis
- Subconjunctival haemorrhage
Scope
This guideline describes the assessment and management of patient’s suffering with acute red eye in a forward medical context or deployed hospital setting.
There are multiple causes of eye pain and redness. Care should be taken when assessing the red eye as it can be difficult to differentiate between diagnoses. If in doubt, request senior clinical review or seek remote reach back when possible.
This guideline does not describe how to conduct an eye examination nor the technique of ophthalmoscopy.
Separate CGOs exist on the following linked topics:
Audience
This guideline is intended for the use of registered healthcare professionals fulfilling a role in a forward medical location or in an emergency department on deployed operations
Initial Assessment & Management
BackgroundRed eye is a common clinical presentation in both the home base and on exercise/operations/deployment.
Many practitioners may not frequently assess eyes but a simple structured approach can enable the exclusion of critical/emergency pathology and management of common urgent care ophthalmological issues.
Assessment should include a thorough history and examination of the patient and their affected eye(s).
Visual acuity should always be assessed and documented (pragmatic assessment should be used in the deployed environment in the absence of a formal Snellen chart.
Fluorescein staining with cobalt blue light examination should be routine practice
Prevention is also important, including use of service eye protection and eye hygiene. Practitioners should incorporate advice on preventative strategies in all red eye consultations.
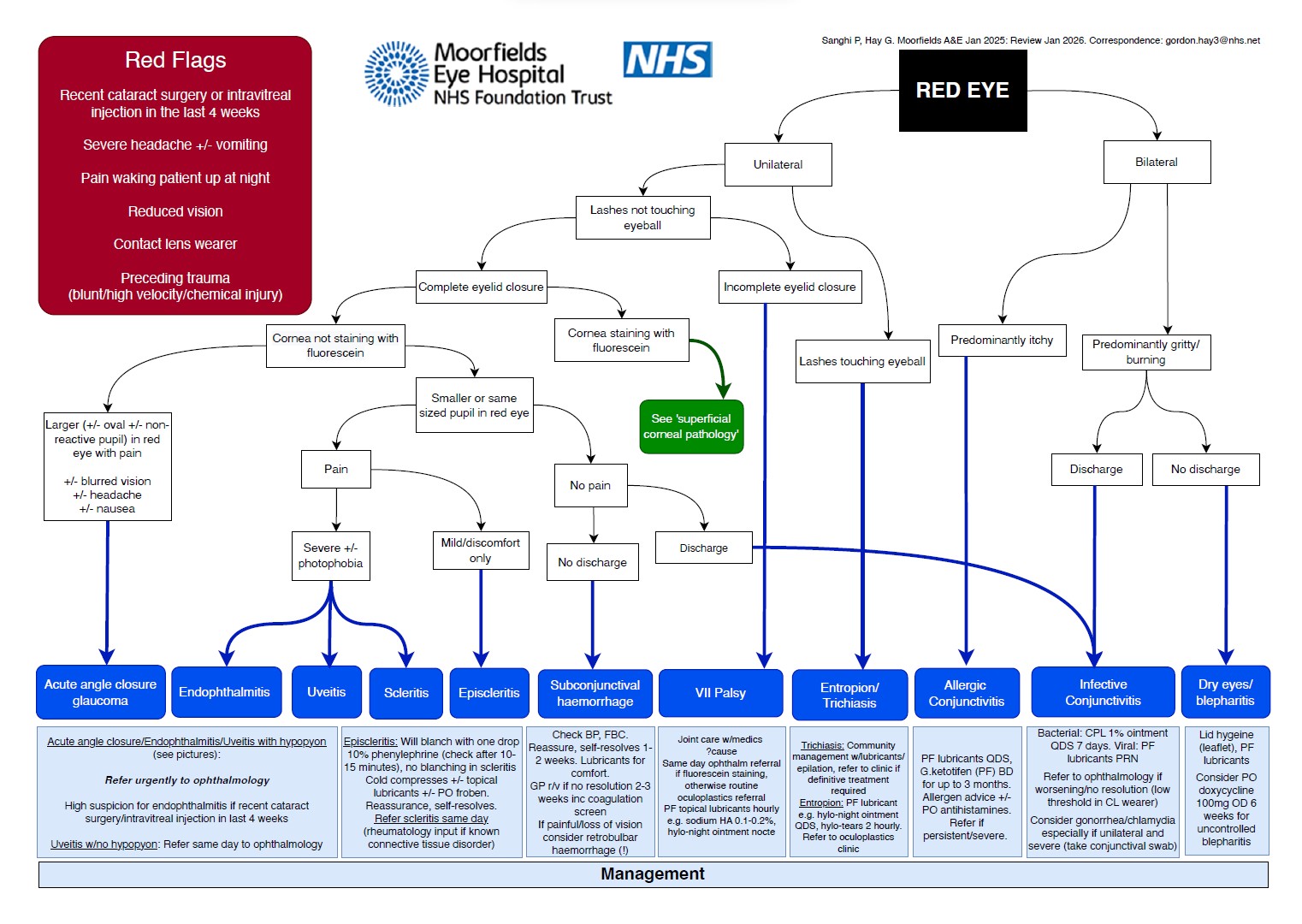
Red FlagsThe following are key indicators of patients with higher risk or emergent presentations:
- Reduced visual acuity
- Severe headache +/- vomiting
- Eye pain waking patient at night
- Preceding eye trauma (blunt, penetrating/high velocity, chemical)
- Contact lens wearer
- (Less than 4 weeks since ocular surgery or intravitreal injection)
Management of the following four common presentations is included in this CGO. Wider information can be found in the Moorfields Eye Hospital guidelines found in the accordion content section.
Conjunctivitis
Conjunctivitis is the inflammation of the eye’s clear lining (conjunctiva). The predominant symptoms are a purulent discharge/watering, red eye and eyelid swelling. It can be difficult to differentiate between bacterial, viral and allergic conjunctivitis.
Bacterial conjunctivitis typically causes:
- Unilateral symptoms (may spread to the other eye within 24-48 hours).
- Lid oedema.
- Watering and purulent discharge.
- Unaffected cornea.
- Unaffected vision (other than by possible transitory blurring that is resolved by blinking).
- Unaffected eye movements.
- Should NOT be any light sensitivity (photophobia)
Both viral and bacterial conjunctivitis will benefit from cool compression on the eye to aid with swelling (e.g. cotton wool pad with sterile water).
Viral conjunctivitis typically lasts for up to 6 weeks, in contrast to bacterial conjunctivitis which persists 5-7 days before improvement.
If bacterial conjunctivitis is suspected, topical antibiotics should be administered as per current deployed antimicrobial guidelines.
Topical lubricants may be helpful for symptomatic relief.
If allergic conjunctivitis is suspected oral antihistamines and topical anti-mast cell drops (e.g. Sodium cromoglycate) should be administered.
Infective conjunctivitis is highly contagious. Frequent handwashing is required and avoid sharing pillows, towels or wash kits. Particular caution should be taken around the use of topical lubricants which must be single patient use.
Many cases can be managed in situ and will not require evacuation on clinical grounds (Tactical situation may still override this e.g. inability to use personal weapon system effectively due to blurring of vision).
Evacuation should be considered where there are red flags, severe cases or where there is resistance to first line treatment.
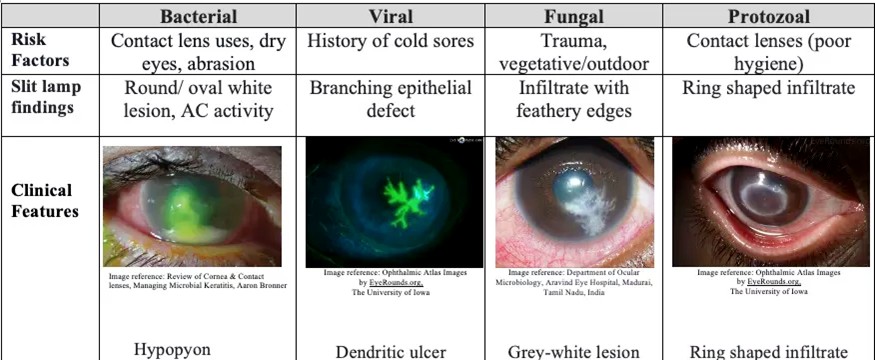
Keratitis
Keratitis is the inflammation of the cornea (the clear dome shaped tissue on the front of the eye covering the pupil and iris).
Keratitis typically causes:
- Unilateral, deep pain.
- Significant photophobia
- Reduced visual acuity.
- Red eye with the sensation of a foreign body within the eye.
- Eye watering/discharge are common.
- A white spot or ‘opacity’ may be visible on the cornea.
- A hypopyon may be visible in cases caused by bacterial infection.
Use of fluorescein staining will reveal a lesion over the cornea, often green in colour whilst under a blue light source. The shape of the stained lesion can suggest the cause of the infection, as demonstrated in the image in the accordion content.
If contact lenses are worn, remove immediately and cease further use.
Commence topical antibiotics as per current deployed antimicrobial guidelines.
Evacuation is required for urgent review by an ophthalmologist – this is a vision-threatening condition.
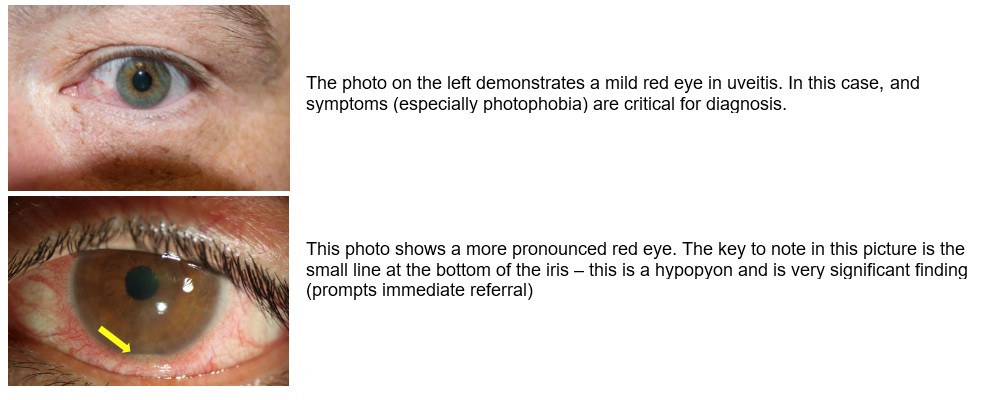
Uveitis
Uveitis is a condition describing inflammation of the iris, ciliary body and choroid. Uveitis often reoccurs in patients, so ensure to ask if they have had similar symptoms previously. Uveitis is associated with other autoimmune inflammatory conditions.
Symptoms can develop acutely or chronically and can be unilateral or bilateral.
Uveitis typically causes:
- Increased sensitivity to light
- Blurred/decreased vision
- Ocular pain
- Watering and redness of the eye(s).
- Eye described as feeling bruised when their eyelid is closed and pressure is applied.
- Often experience increased pain when their ciliary muscle is contracting (e.g. when reading).
- Pupil often small and may not fully dilate compared to the other eye.
- No pain on movement of the eye.
- No restriction of eye movement.
There is no fluorescein staining of the cornea. Pictures of typical presentations can be found in the accordion content.
There is no deployed treatment for uveitis, however if the diagnosis is in doubt commence topical antibiotics as per current deployed antimicrobial guidelines to cover for other causes of acute red eye.
Evacuation is required for urgent review by an ophthalmologist – this is a vision-threatening condition.
Subconjunctival Haemorrhage
Subconjunctival haemorrhage is a bleed beneath the conjunctiva. Often the conjunctiva will appear raised with the blood.
It is usually asymptomatic and can occur spontaneously (for example after vomiting/coughing/straining) or after minor trauma.
Vision is unaffected and there is usually no pain.
Subconjunctival haemorrhages should resolve spontaneously without any intervention. Ensure to check the patient’s blood pressure and if normal, reassure the patient that the eye should self-resolve over 1-2 weeks.
If pain commences or increases, they should represent for further review.
Advanced Assessment & Management
Conjunctivitis
Ensure the both eyelids have been everted and a thorough check completed for foreign bodies.
Use of the slit lamp is recommended to confirm the cornea is clear and there is no evidence of keratitis.
Keratitis
Slit lamp assessment is recommended, along with early referral/discussion with ophthalmology.
Do not start topical steroids without specific ophthalmology advice
Uveitis
Slit lamp assessment is recommended, along with early referral/discussion with ophthalmology.
Mydriatics (eg. tropicamide 0.5%) and steroid eye drops are the mainstay of treatment.
Basic bloods, faecal calprotectin (if suspecting IBD), infective screens (TB, lyme, HIV, syphilis, HSV/VZV) and autoimmune screens (HLA-B27, ANA, rheumatoid factor), if available, will be useful.
If uveitis is found to be caused by systemic disease, treatment of the disease may relieve eye symptoms.
Prolonged Casualty Care
Regular review should be undertaken including assessment of visual acuity.
Maintain strict antibiotic dosing regimes if initiated and monitor for signs of resistance / treatment failure.
Manage light sensitivity with a dark environment or sunglasses.
Regular cool compression and gentle washing of the eye using sterile water soaked gauze/cotton wool pads may be of benefit for many conditions.
Paediatric Considerations
Conjunctivitis
Paediatric conjunctivitis is very common.
Management is the same as for adult patients.
Keratitis
High risk of amblyopia (lazy eye) if symptoms are not resolved quickly.
Neonates (<1 month) with purulent discharge may have gonococcal keratitis – treatment is with ceftriaxone.
Uveitis
Uveitis in children is often asymptomatic and presents in a “white eye” without redness or pain.
Always consider Juvenile Idiopathic Arthritis (JIA) as an underlying cause and ensure screening is arranged if appropriate.
Uveitis is also associated with inflammatory bowel disease, sarcoidosis and Behcet's syndrome.
Subconjunctival Haemorrhage
Evaluate for non-accidental injury if the history is inconsistent or there are any suspicious findings.
Subconjunctival haemorrhage is common in newborns following vaginal delivery (due to pressure changes in birth canal). This is benign and typically resolves within 1-2 weeks without treatment.