The app and website was publicly released on 2 Apr 2024
Update Jan 2025
The content continues to undergo review by all our cadres.
The content remains subject to the following provisos: - The content will be subject to continuous update and review - Old content (from previous CGOs) will be converted into the new format, using the new tools and layouts - Content may be moved around - The layout will change and reflect the needs of the user - Content will be created - Content may be deleted/retired
CGO development will continue.
Saf [Updated 21 Jan 2025]
Acute Compartment Syndrome & Fasciotomy
!Warning
What's new / Latest updates
This is the first iteration of this CGO
Objectives
This guideline covers the diagnosis of acute compartment syndrome and procedural guidance for the treatment, which is urgent surgical fasciotomy of the affected limb(s).
Scope
This guideline covers all echelons of deployed surgical care (i.e. R2 and higher).
Audience
The target audience is deployed surgical teams.
Initial Assessment & Management
Background: The muscles of the limbs are contained within fascial compartments. These compartments will prevent expansion of the muscles if they swell. In the context of deployed military care this is usually secondary to trauma or reperfusion injury but may also be due to electrocution injury or burns.
When the pressure in the compartment exceeds the capillary perfusion pressure muscle ischaemia and ultimately muscle death will occur. This is known as acute compartment syndrome. This condition can also be caused by dressings and plaster-casts that are applied too tightly or which become tight due to limb swelling.
Fasciotomy is the process of incising the tough fascia to relieve the pressure in the compartment and restore perfusion to the tissues.
Fasciotomy is indicated in long bone fractures when the onset of compartment syndrome is suspected, after revascularisation of a limb, and after high voltage electrical burns. Fasciotomy is most commonly performed on the leg but can be done on the thigh, arm, forearm and hand. Fasciotomy of the foot is controversial and rarely indicated in the deployed setting.
Diagnosis
In the deployed setting this is a clinical diagnosis. The decision to perform fasciotomy must be made in the context of the resource limitations on the surgical team and the evacuation timelines to the next surgical facility.
Failure to perform this procedure on a patient with compartment syndrome will lead to functional loss or amputation
The Awake patient
Severe unremitting pain out of proportion to the injury is the hallmark clinical finding. Severe pain on passive stretch of the muscles running in the compartment can add weight to the diagnosis but is not always reliable. Do not wait for signs of vascular compromise (pallor, pulselessness, cold extremity, distal weakness and numbness), pulse may continue to be palpable in compartment syndrome. Numbness in the first web space (deep peroneal nerve) is described as being indicative of compartment syndrome of the anterior compartment of the leg but this sign is not to be relied upon in isolation. Common causes of acute compartment syndrome in the deployed setting are severe trauma and/or ischaemia from vascular trauma or tourniquet use.
Unconscious Patients
The decision to perform fasciotomies in these patients is made primarily on injury pattern and mechanism of injury. Examination finding of a firm compartment is unreliable. Using the anaesthetic equipment to create a compartment pressure monitor is described in the literature but should not form part of routine deployed surgical care. The guiding principle in unconscious patients is that if the treating team are concerned about compartment syndrome then fasciotomy should be performed without delay.
All Patients
Any patient with limb ischaemia (tourniquet, vascular injury, etc) longer than 6 hours should undergo fasciotomy of compartments distal to the point of ischaemia. The 6-hour limit is based on convention rather than strong evidence so deviation may be made based on clinical judgement and fasciotomy after significantly shorter ischaemic time is supported. The longer the evacuation timeliness from the surgical facility, the lower the threshold should be for performing fasciotomy, both in terms of ischaemic time and diagnostic confidence.
Non-surgical management
in awake patients where the likely cause is due to tight dressings or a plaster cast, the immediate management is to release the compressing layers down to skin. The patient is then monitored carefully. If their pain resolves significantly upon releasing the layers then a non-operative management plan may be considered. Alternative methods of controlling unstable extremity fractures will need to be performed such as external fixation or traction.
Delayed Presentation Beyond 8 Hours
The management of patients with missed or delayed presentation of acute compartment syndrome is controversial. This is because the muscles and nerves in the compartment are likely to be irreversibly damaged after 8 hours. In this context, creating large surgical wounds that may become infected may commit the patient to amputation. Late fasciotomy for delayed presentation or missed diagnosis of compartment syndrome is associated with a high amputation rate. The literature does not provide clear guidance for what is defined as “late” nor what is the best way to manage these patients. Therefore the senior clinical decision-makers present must use their judgement in this situation, taking into account all of the contextual factors of the deployed setting.
Advanced Assessment & Management
Fasciotomy - Surgical Guidelines
Equipment Required
Surgical Instruments (see Fig 1):
10 Blade
McIndoe scissors
Forceps, toothed, large & small (Gillies & Lanes)
Diathermy
Mayo scissors
Fig 1. Surgical equipment for fasciotomy
For the Dressing
Non-adherent base layer
Velband
Crepe
POP if necessary to stabilise limb
Patient Position
Supine/Crucifix, arm boards to be used. All dressings/splints should be removed for prep. The limb should be socially washed prior to prep. Betadine and water in a bowl with large swabs can be used for this social wash.
Prep and Drape
Prep beyond joints above and below limb for fasciotomy. Limb to be elevated for circumferential preparation. U-drapes to be fashioned from universal drapes and applied above proximal joint, a cut off drape or glove to cover extremity beyond distal joint.
Surgical Approaches
In all cases, the length of the fasciotomy incisions must be the full length of the affected compartment.
All necrotic tissue must be excised according to the principles described in the wound excision CGO.
Closure
Do not close fasciotomy wounds in the forward (Role 2) deployed setting unless there are strong contextual reasons to do so (see Prolonged Field Care below).
Do not use sloops to partially close fasciotomy wounds. Standard dressing with a non-adherent layer then velband and crepe is acceptable.
If available, negative pressure dressings can be used but are not essential in this setting. Fasciotomy patients with negative pressure dressings must be monitored closely as these dressings can, rarely, induce secondary compartment syndrome due to their mode of action. In these cases, the vacuum must be immediately released and not reintroduced for at least 48 hours.
Post-Operative Management
Analgesia
Post-op bloods (Hb, renal function if available)
Antibiotics (1.2 g Co-Amoxiclav IV TDS) until definitive closure
Plan for return to theatre for relook and/or closure within 48-72 hours, ideally at Role 3
Evacuate via stretcher
Prolonged Casualty Care
Wound Care
If the dressings adequately control wound exudate and post-op bleeding then they should be left undisturbed until second look in theatre in 48-72 hours. Excessive bleeding might require a return to theatre to identify the source.
Further Surgery
If second-look surgery is required, the timing will be driven by operational context but should be no longer than 72 hours after initial surgery. If the wounds are found to be healthy at second look then closure may be considered. If direct closure of both wounds is not possible, consider closing one side and re-dressing the other. In cases where the wounds cannot be closed, the options are 1. allowing the wound to heal by secondary intention or 2. repatriation to Role 4 for definitive surgical management.
Paediatric Considerations
Within the context of deployed surgical care, there are no practical differences between adults and children in terms of the management of acute compartment syndrome.
Note, however, that compartment syndrome is comparatively rare in children and that children externalise pain differently to adults so the diagnosis may be more challenging than in adults.
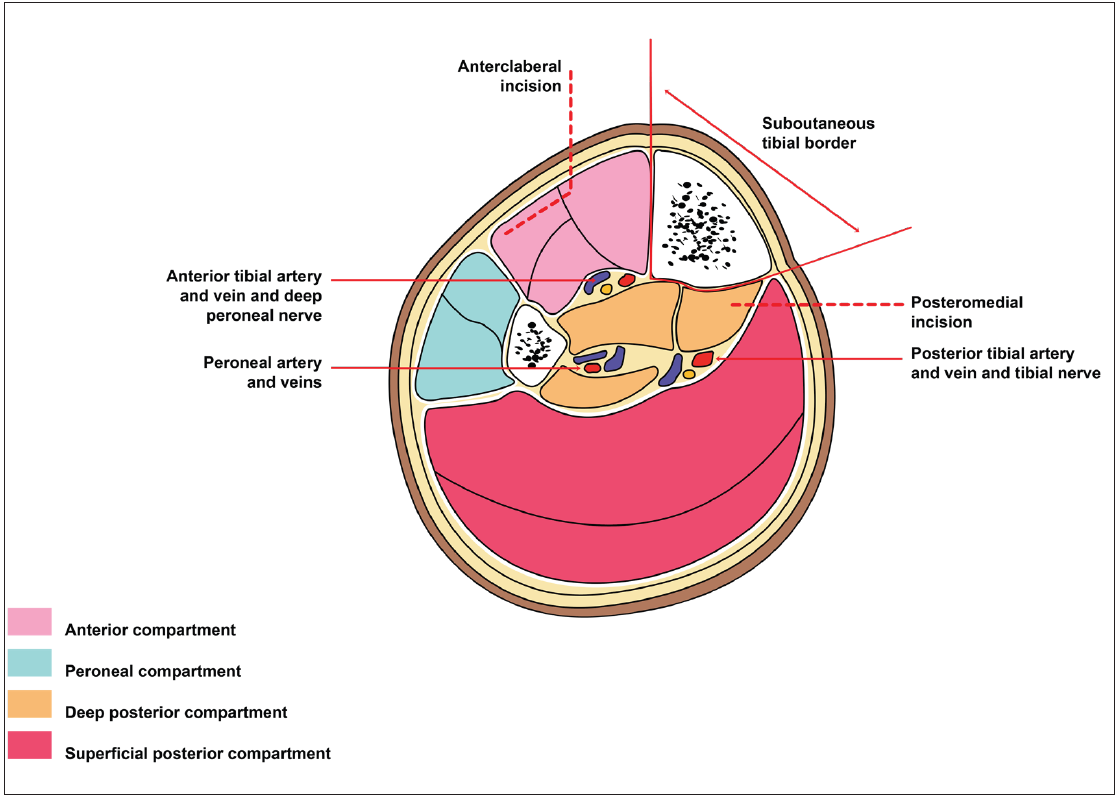
Fasciotomy of the Leg
The green dotted line (Fig 2) represents the palpable subcutaneous border of the tibia. The blue lines represent the planned incisions with the medial one being 1.5cm medial to the medial subcutaneous border of tibia and the lateral one being 2cm lateral to the lateral subcutaneous border of the tibia. The red crosses represent the position of the medial perforating vessels supplying the skin (5, 10, 15 cm above the medial malleolus). These must be avoided as they supply the skin on the medial side of the leg and may be necessary for future plastic surgical reconstruction. The blue line is the incision used by the surgeon to perform fasciotomy.
Fig. 2 Leg fasciotomy incisions - note that these must be full length of the affected compartment. Do not take the length of the lines in this diagram as indicative of length, they are for position and orientation guidance only.
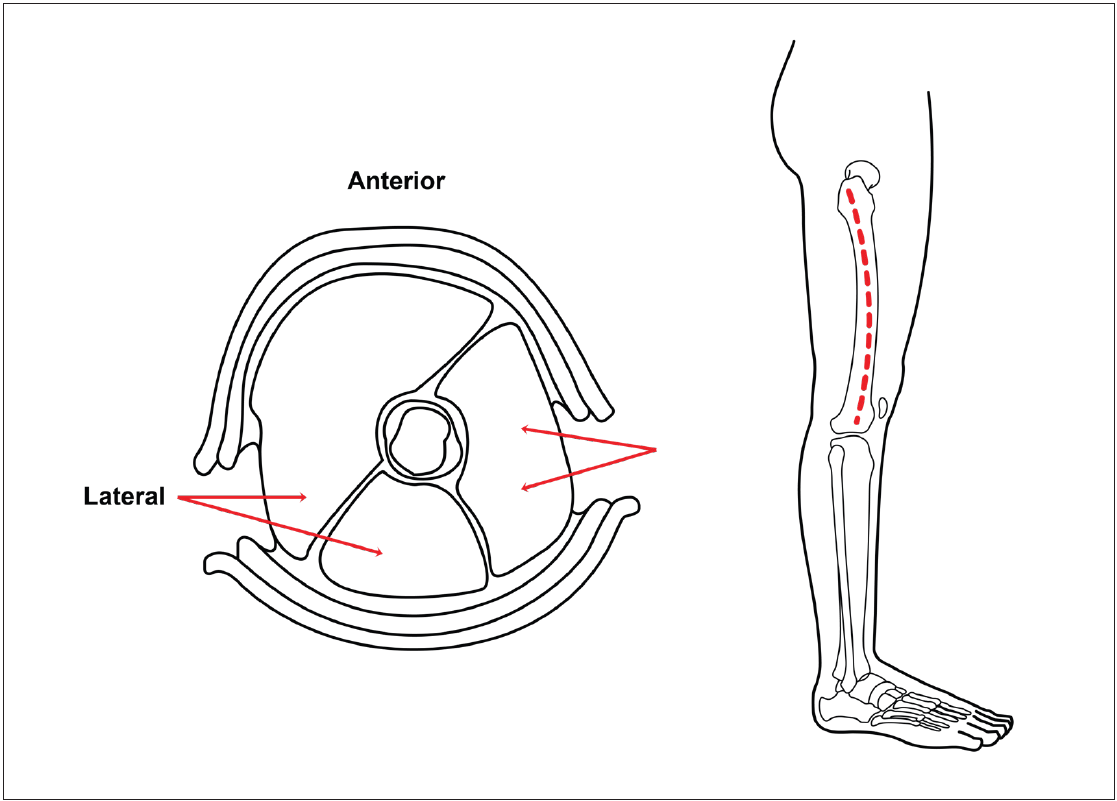
The dotted line (Fig 3) represents the approach to the peroneal compartment and deep posterior compartment from the initial incisions.
Fig 3. The leg is decompressed via two incisions. The medial incision decompresses the deep and superficial posterior compartments. Note that gastrocnemius and soleus must be taken off the back of the tibia in order to allow full decompression of the deep posterior compartment. The anterior and peroneal compartments are decompressed via the lateral incision.
Fasciotomy of the Thigh
Fig 4. The thigh is decompressed via two incisions. The anterior compartment is decompressed through the lateral incision. Vastus lateralis is lifted and the lateral intermuscular septum is incised to decompress the posterior compartment. The adductor compartment is decompressed via the medial incision.
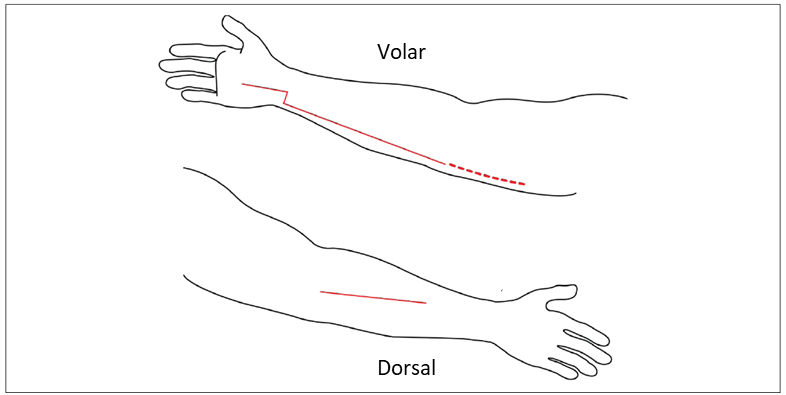
Fasciotomy of the Arm
Fig 5. The forearm is decompressed via two incisions one volar/ulnar incision and one radial/dorsal incision. The volar/ulnar incision starts in the hand with a carpal tunnel release and then deviates ulnarly across the wrist creases. It is extended along the ulnar/volar aspect of the forearm to end at a point 1/4 of the way across the antecubital fossa. All volar muscle groups are released via this incision. Adequacy of deep distal dissection is confirmed when pronatus quadratus is appreciated. The dorsal/radial incision is aligned along the border between the mobile wad and the extensor compartment and is used to decompress both.
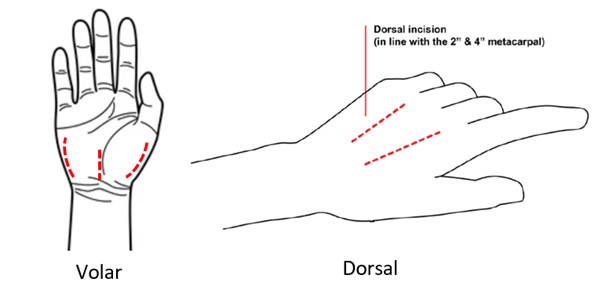
Fasciotomy of the Hand
Fig 6. Five incisions are required to decompress the hand. Two dorsal incisions, centred oved the 2nd and 4th metacarpals are used to decompress both the dorsal and volar interossei. Three volar incisions are used to decompress the thenar muscles, the carpal tunnel, and the hypothenar muscles.
British Orthopaedic Association Standards in Trauma: Diagnosis and Management of Compartment Syndrome of the Limbs
Glass GE, Staruch RM, Simmons J, Lawton G, Nanchahal J, Jain A, Hettiaratchy SP. Managing missed lower extremity compartment syndrome in the physiologically stable patient: A systematic review and lessons from a Level I trauma center. Journal of Trauma and Acute Care Surgery. 2016 Aug 1;81(2):380-7.
Lundy DW, Bruggers JL. Management of missed compartment syndrome. Compartment Syndrome: A Guide to Diagnosis and Management. 2019:105-12.
Barker T, Midwinter M, Porter K. Monitoring and interpreting compartment pressures in acute compartment syndrome. Trauma. 2012;14(2):163-168. doi:10.1177/1460408611432098
Necessity, Role, and Outcomes of Fasciotomy in Patients with Acute Limb Ischemia. Natour, Abdul Kader et al. Annals of Vascular Surgery, Volume 94, 143 - 153