
{kind=link}
Hypoglycaemia
Warning
Objectives
Guide safe pragmatic management of hypoglycaemia in deployed settings
Scope
How do I manage hypoglycaemia on Ops?
Audience
Role 1 to 3.
Trained healthcare providers
Initial Assessment & Management
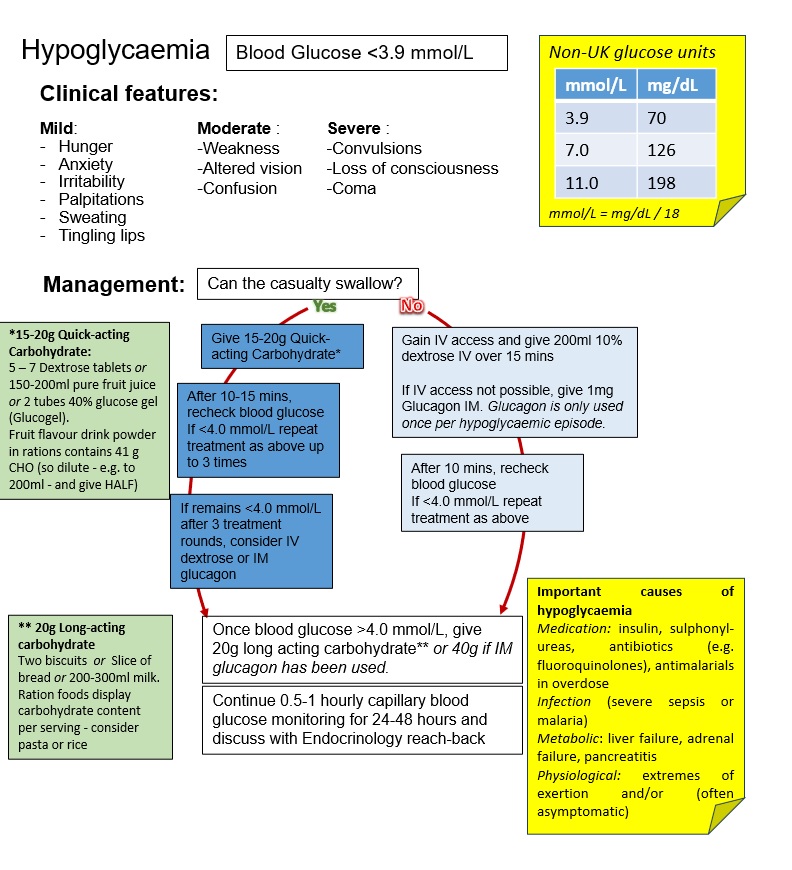
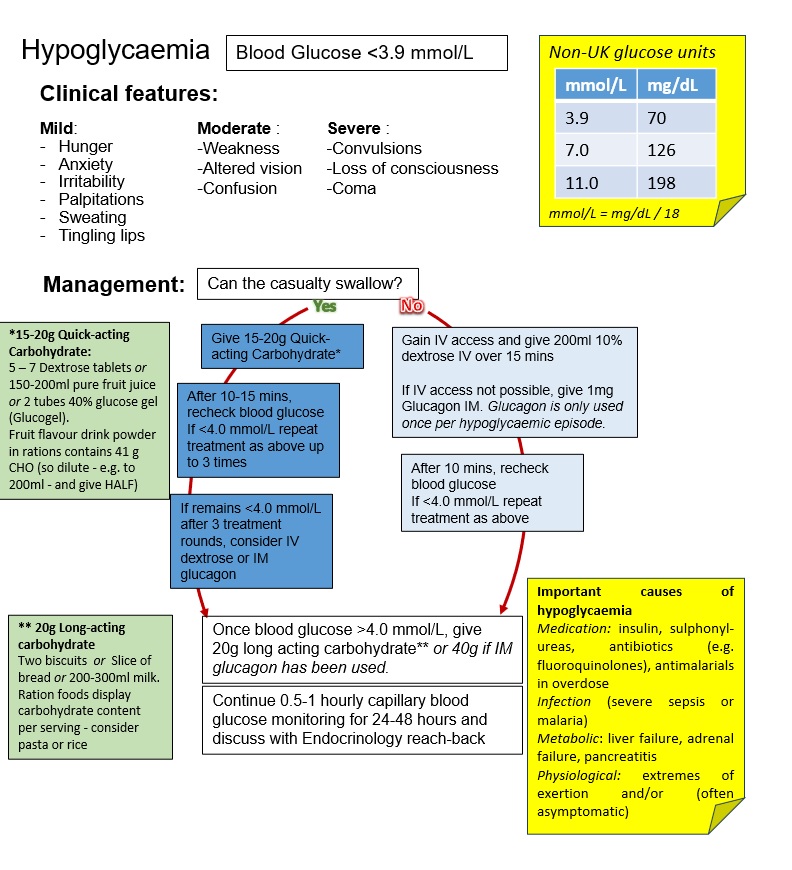
Non-UK Glucose Units
|
mmol/L |
mg/dL |
|
3.9 |
70 |
|
7.0 |
126 |
|
11.0 |
198 |
Hypoglycaemia
You may prefer the hypoglycaemia algorithm designed to print on a single side of A4, here
This is a low blood glucose level (BGL) < 3.9 mmol/L (70 mg/dL) in the presence of clinical features, which resolve after treatment of the low BGL.
Clinical features
| Mild | Moderate | Severe |
| Hunger | Weakness | Confulsions |
| Anxiety | Altered vision | Loss of consciousness |
| Irritability | Confusion | Coma |
| Palpitations | ||
| Sweating | ||
| Tingling lips |
Management
Can the patient swallow?
YES:
- Give 15-20g Quick-acting Carbohydrate:
- 5 – 7 Dextrose tablets or
- 150-200ml pure fruit juice or 2 tubes 40% glucose gel (Glucogel)
- Fruit flavour drink powder in rations contains 41 g CHO (so dilute - e.g. to 200ml - and give HALF)
- Follow this up immediately with 20g long-acting carbohydrate:
- Two biscuits or Slice of bread or 200-300ml milk.
- Ration foods display carbohydrate content per serving - consider pasta or rice
- After 10-15 min, recheck BGL.
- If <4.0 mmol/L, repeat first 2 steps up to 3 times
- If BGL remains below 4.0 mmol/L consider IV dextrose or IM glucagon.
NO:
- Gain IV/IO access and give 200ml 10% dextrose IV over 15 mins
- If IV/IO access not possible, give 1mg Glucagon IM. Glucagon is only used once per hypoglycaemic episode
- 2. After 10 mins, recheck blood glucose
- If <4.0 mmol/L repeat treatment as above.
- When conscious follow up with oral long-acting carbohydrate as above
Advanced Assessment & Management
Important causes of hypoglycaemia
Medication: Insulin, sulphonyl-ureas, antibiotics (e.g. fluoroquinolones), antimalarials in overdose
Infection: (severe sepsis or malaria)
Metabolic: Liver failure, adrenal failure, pancreatitis
Physiological: Extremes of exertion and/or exertional heat illness (often asymptomatic)
Prolonged Casualty Care
Hypoglycaemia
Once blood glucose >4.0 mmol/L, give 20g long acting carbohydrate or 40g if IM glucagon has been used.
Continue 1-2 hourly capillary BGL until these are consistently above 5 mmol/L (90 mg/dL) for 4 hours.
Paediatric Considerations
Hypoglycaemia
Children have increased risk of recurrent hypoglyacemia. Monitor closely.
Calculate the appropriate amount of glucose to administer based on the child's weight and age.
Oral treatment: Give 0.3 g/kg fast acting carbohydrate (9g of glucose for a 30kg child, 15g for a >50kg child). Follow up with 10-15g carbohydrate snack
Glucagon: If the child is less than 25kg, give 0.5mg. If 25kg or over give 1mg. Can be repeated once.
IV glucose: give 2-5 ml/kg 10% intravenous dextrose. Repeat if unresposive.
All severely malnourished children are at risk of hypoglycaemia and, immediately on admission, should be given a feed, or glucose or sucrose solution.
If the child is conscious and able to drink, glucose or sucrose should be given orally or by nasogastric tube followed by small and frequent feedings with F-75 therapeutic milk.
If the child is unconscious, glucose should be given intravenously, or glucose or sucrose by nasogastric tube. When the child regains consciousness, small and frequent feedings with F-75 therapeutic milk should be started.
All malnourished children with suspected hypoglycaemia should also be treated with broad-spectrum antimicrobials for serious systemic infection.