{kind=link}
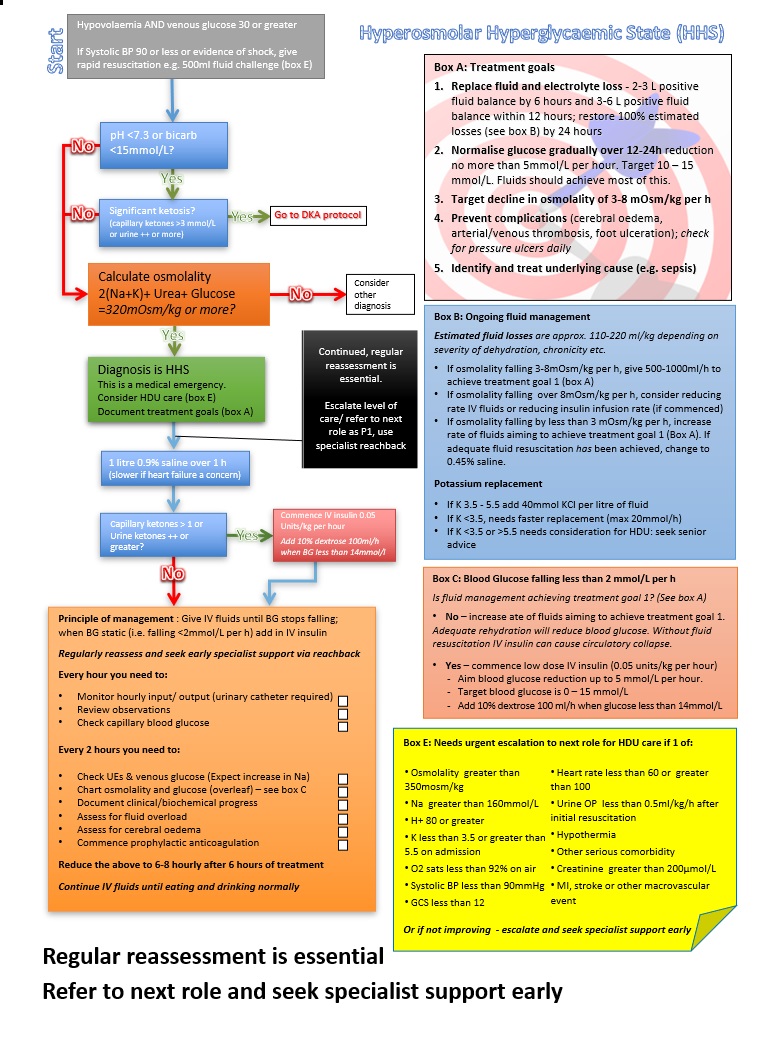
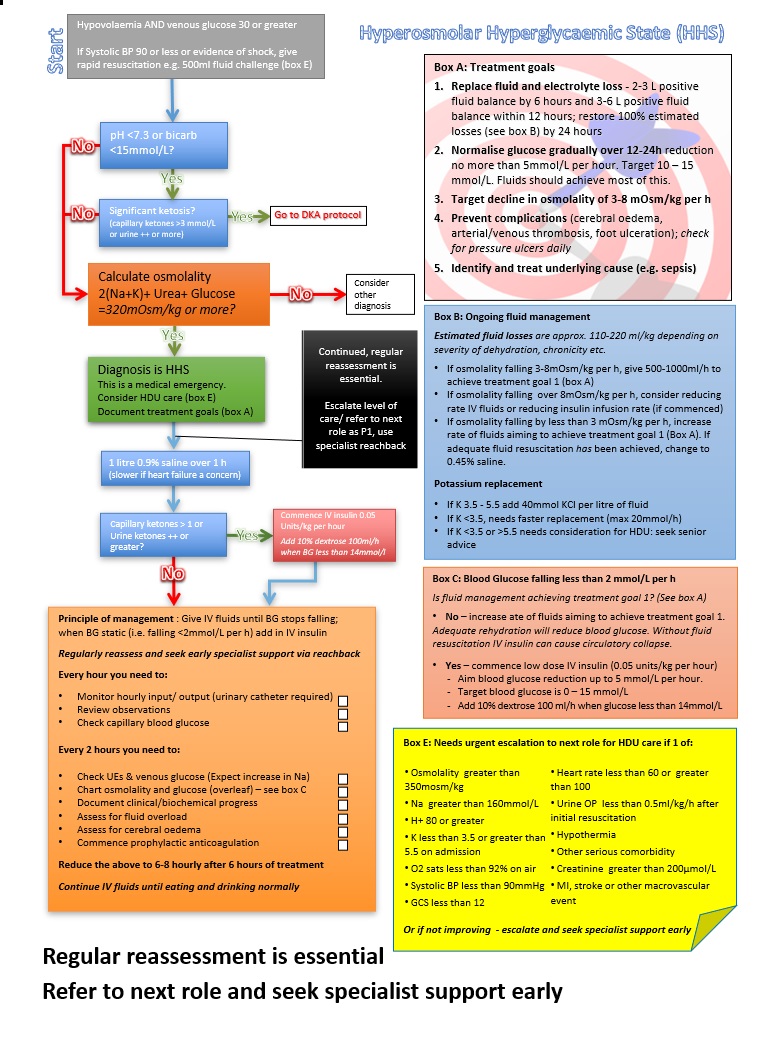
- Osmolality greater than 350mosm/kg
- Na greater than 160mmol/L
- H+ 80 or greater
- K less than 3.5 or greater than 5.5 on admission
- O2 sats less than 92% on air
- Systolic BP less than 90mmHg
- GCS less than 12
- Heart rate less than 60 or greater than 100
- Urine OP less than 0.5ml/kg/h after initial resuscitation
- Hypothermia
- Other serious comorbidity
- Creatinine greater than 200μmol/L
- MI, stroke or other macrovascular event
Hyperosmolar hyperglycaemic state (HHS)
Warning
Objectives
Safely manage HHS on Ops
Scope
How do I manage the patient with very high blood glucose level (>30 mmol/L / 540 mg/dL) AND hypovolaemia AND osmolality of 320 mmol/L or higher?
Audience
Trained HCPs
Initial Assessment & Management
You may prefer the HHS algorithm designed to print on a single side of A4, here
Non-UK glucose unit conversion
|
mmol/L |
mg/dL |
|
3.9 |
70 |
|
7.0 |
126 |
|
11.0 |
198 |
If Systolic BP 90 or less or evidence of shock, give rapid resuscitation e.g. 500ml fluid challenge (box E)
Check ketones and blood gas. pH <7.3 or bicarb <15mmol/L AND ketosis (dipstick '++' or greater; capillary ketones >3 mmol/L) - Use Diabetic Ketoacidosis (DKA)
Calculate osmolality (2 × (Na+K) + Urea + Glucose)
320mOsm/kg or more?
YES - Diagnosis is HHS. This is a medical emergency. Consider HDU care. Document treatment goals.
Give 1 litre 0.9% saline over 1 h (slower if heart failure a concern)
Advanced Assessment & Management
If capillary ketones > 1 or Urine ketones ++ or greater, commence IV insulin 0.05 Units/kg per hour. Add 10% dextrose 100ml/h when BG less than 14mmol/l
Document estimated fluid losses - approx. 110-220 ml/kg depending on severity of dehydration, chronicity etc.
- If osmolality falling 3-8mOsm/kg per h, give 500-1000ml/h to achieve treatment goal 1 (box A)
- If osmolality falling over 8mOsm/kg per h, consider reducing rate IV fluids or reducing insulin infusion rate (if commenced)
- If osmolality falling by less than 3 mOsm/kg per h, increase rate of fluids aiming to achieve treatment goal 1 (Box A). If adequate fluid resuscitation has been achieved, change to 0.45% saline.
Potassium replacement
- If K 3.5 - 5.5 add 40mmol KCl per litre of fluid
- If K <3.5, needs faster replacement (max 20mmol/h)
- If K <3.5 or >5.5 needs consideration for HDU: seek senior advice
Prolonged Casualty Care
Ongoing management of HHS is intensive. Consider referring to next role at earliest opportunity
Principle of management : Give IV fluids until BG stops falling; when BG static (i.e. falling <2mmol/L per h) add in IV insulin
Regularly reassess and seek early specialist support via reachback
Every hour you need to:
- Monitor hourly input/ output (urinary catheter required)
- Review observations
- Check capillary blood glucose
Every 2 hours you need to:
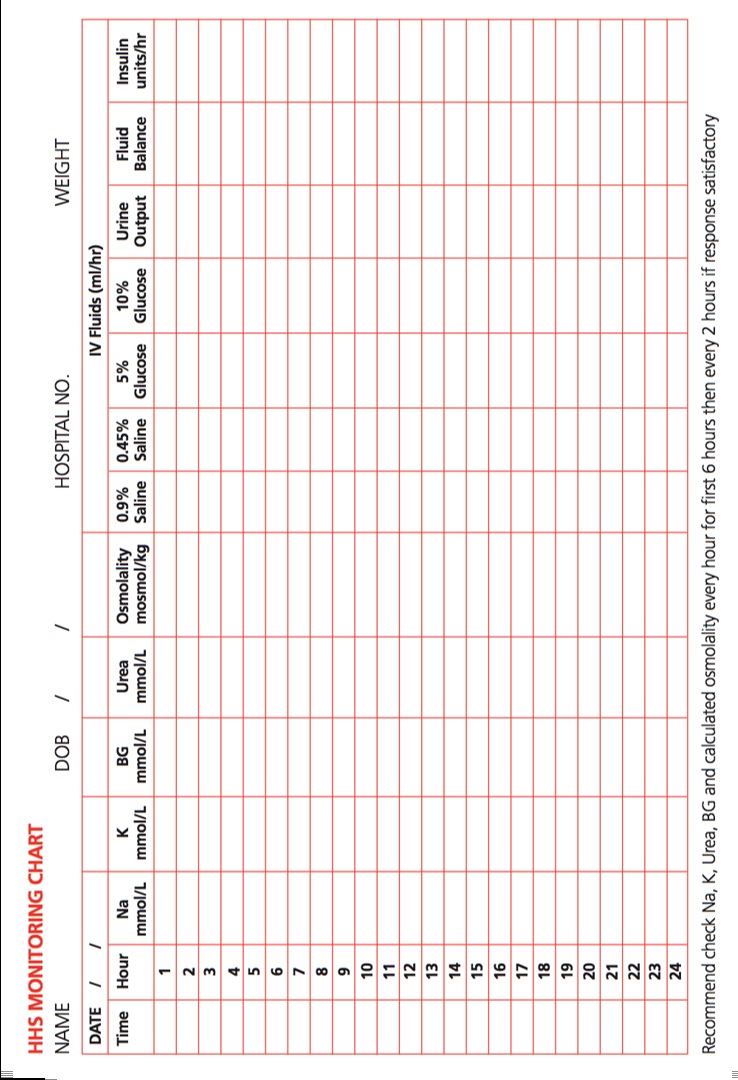
- Check UEs & venous glucose (Expect increase in Na)
- Chart osmolality and glucose (overleaf) – see 'blood glucose falling < 2mmol/L per h' if relevant
- Document clinical/biochemical progress
- Assess for fluid overload
- Assess for cerebral oedema
- Commence prophylactic anticoagulation
Reduce the above to 6-8 hourly after 6 hours of treatment
Continue IV fluids until eating and drinking normally
1.Replace fluid and electrolyte loss - 2-3 L positive fluid balance by 6 hours and 3-6 L positive fluid balance within 12 hours; restore 100% estimated losses (see box B) by 24 hours
2.Normalise glucose gradually over 12-24h reduction no more than 5mmol/L per hour. Target 10 – 15 mmol/L. Fluids should achieve most of this.
3.Target decline in osmolality of 3-8 mOsm/kg per h
4.Prevent complications (cerebral oedema, arterial/venous thrombosis, foot ulceration); check for pressure ulcers daily
5.Identify and treat underlying cause (e.g. sepsis)
Is fluid management achieving treatment goal 1? (See box A)
- No – increase ate of fluids aiming to achieve treatment goal 1.
Adequate rehydration will reduce blood glucose. Without fluid resuscitation IV insulin can cause circulatory collapse.
- Yes – commence low dose IV insulin (0.05 units/kg per hour)
- Aim blood glucose reduction up to 5 mmol/L per hour.
- Target blood glucose is 0 – 15 mmol/L
- Add 10% dextrose 100 ml/h when glucose less than 14mmol/L