
{kind=link}
Hyperkalaemia
Warning
Objectives
Manage hyperkalaemia in the deployed setting
Scope
Hyperkalaemia in R1/R2
Audience
Clinical decision makers R1-R3
Initial Assessment & Management
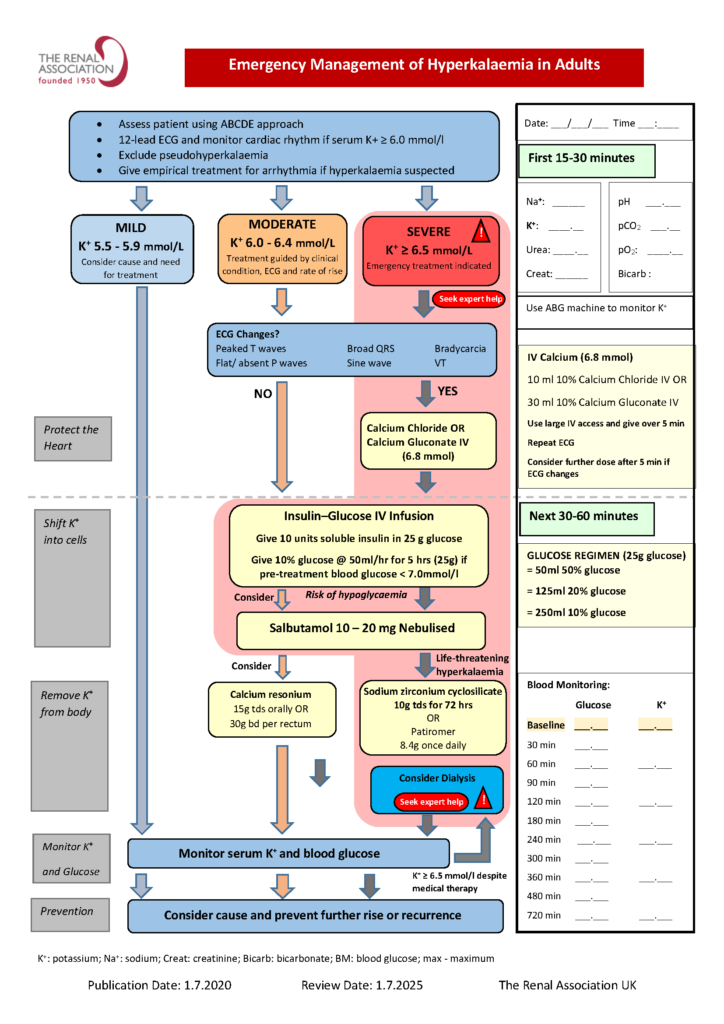
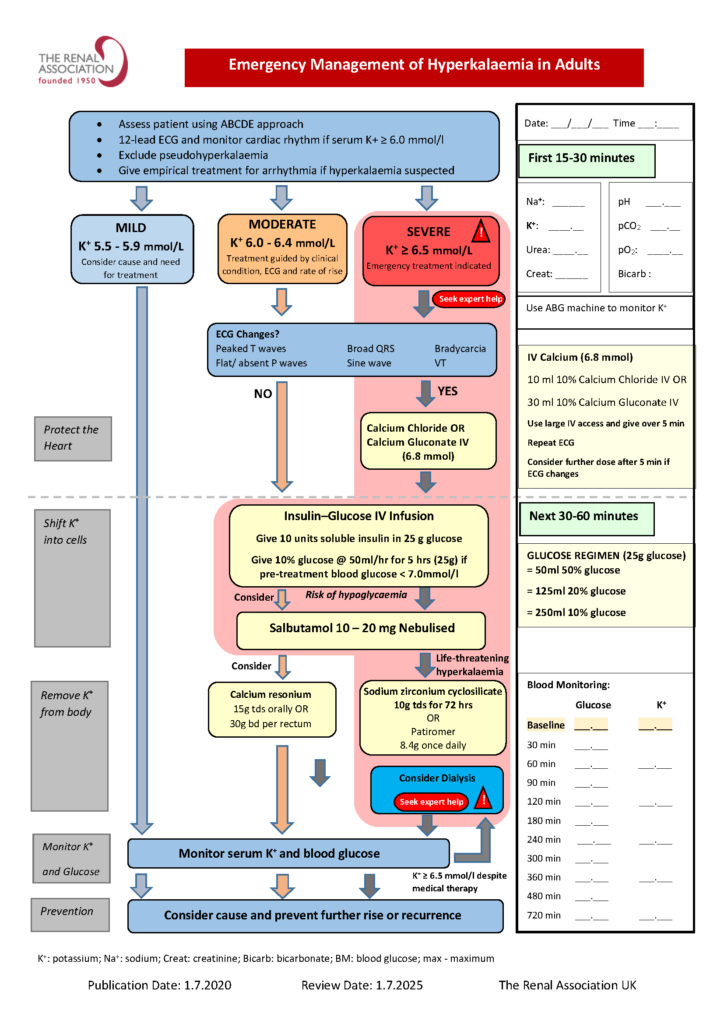
Serum K >6.5 mmol/L or ECG changes: Administer Calcium chloride 10% 10mL via a large bore cannula or central access. This intervention does not aim to lower the potassium, but to stabilise the myocardium. Changes should be seen over 1-3 minutes. If ongoing ECG changes this can be repeated every 10 minutes (up to 50ml). Normalisation may only endure for 30-60 minutes whilst lowering the potassium as below.
ECG changes:
- Peaked T waves
- P wave widening/ flattening
- PR prolongation
- Bradyarrhythmia: sinus bradycardia, slow AF, high-grade AV block
- Conduction block: Bundle Branch block, Fascicular block
- QRS widening
Serum K+ >6.0 mmol/L: Administer insulin-glucose infusion, monitor K+ hourly, monitor urine output, consider salbutamol nebuliser
Insulin-Glucose infusion:
- Mix 25g glucose-containing fluid (e.g. 50mL Glucose 50% or 100ml of 20%) with 10 units Insulin
- Infuse over 5- 30 mins via large bore cannula
- If glucose >15mmol/L then additional glucose with the 10 units of insulin is not necessary, but monitor BMs along with potassium.
Salbutamol Nebuliser:
- This should be nebulised in doses of at least 10mg salbutamol, and again aims at a transient reduction (~2hrs) in potassium.
Advanced Assessment & Management
Additional management:
- 2 large bore IV cannulae
- Urinary catheter and monitor urine output
- Monitor glucose
- Regular/ continuous ECG monitoring
- Salbutamol nebulisers (aid to moving potassium intracellularly)
Salbutamol and insulin utilise ion channels to treat the patient's cells as a reservoir, temporarily shifting dangerously high plasma levels intracellularly. For an enduring treatment, potassium must be removed from the body. This can be using the gut (calcium resonium, effect in hours to days, or sodium Zirconiium cyclosilicate - Lokelma - which takes effect in hours), kidneys (diuresis with potassium wasting diuretics like loop diuretics as an adjunct), or as a last resort, renal replacement therapy.
The Gut:
- In role 3 modules, Calcium resonium is available as Calcium Polystyrene Sulfonate. Its time to effect makes it less immediately helpful than the diuresis, but its mechanism is independent of renal function so it is complimentary and may have some impact particularly whilst awaiting evacuation. Lokelma is not currently available in deployed modules, but awareness is helpful due to to its superior speed of onset.
Hypovolaemic/ Euvolaemic:
- Aim to restore renal perfusion and urine output so potassium can be excreted. Use 0.9% saline 500 mL IV, then reassess BP/perfusion, evidence of volume overload and urine output; repeat if urine output improving and no evidence of fluid overload.
- If anuric after volume repletion, additional fluids will not clear potassium - move early to escalation for RRT while continuing temporising measures.
Hypervolaemic:
- If urine output present or achievable, give trial IV furosemide 40–80 mg IV, then assess urine output and blood pressure response at 60 min. If diuresis is good, this will be achieving potassium loss; repeat potassium levels/VBG hourly initially to assess response, and if downtrending then at 2, 4, 6 and 24 hours after active management.
- The dose can be repeated as necessary when urine output tapers, or switched to a continuous furosemide infusion as per MEDUSA. Forced diuresis should be stopped when potassium is 5.5mmol/l, remembering to re-check potassium as significant shifts from intracellular reservoirs can cause recurrence of hyperkalaemia.
- If there is an inadequate response but confident that patient is hypervolaemic, then escalate dose to 1mg/kg; a failure at this dose suggests the patient's kidneys will not respond to diuresis as a mechanism for potassium removal and renal/ICU is needed to pursue removal of potassium via renal replacement therapy; a service available via CCAST.
- If the patient becomes hypotensive, develops a worsening AKI, or becomes anuric, stop chasing diuresis and seek additional advice via reachback.
Prolonged Casualty Care
Refractory hyperkalaemia without urine output will require removal of potassium via renal replacement therapy which is a service available via CCAST.