Update Jan 2025
The content continues to undergo review by all our cadres.
The content remains subject to the following provisos:
- The content will be subject to continuous update and review
- Old content (from previous CGOs) will be converted into the new format, using the new tools and layouts
- Content may be moved around
- The layout will change and reflect the needs of the user
- Content will be created
- Content may be deleted/retired
CGO development will continue.
Saf
[Updated 21 Jan 2025]
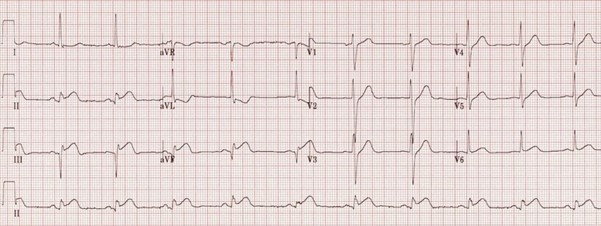
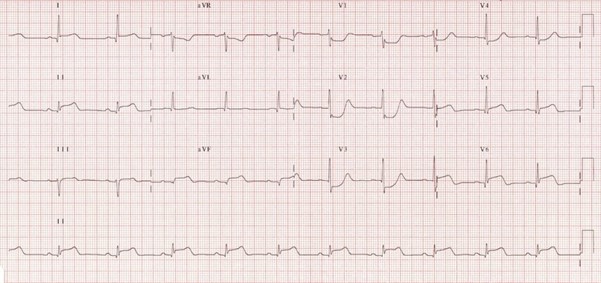
To outline the management of patients presenting to deployed medical facilities with chest pain which is then confirmed to be ST elevation myocardial infarction (STEMI).
This guideline intends to cover the initial investigations and management of patients presenting to the deployed medical treatment facilities with cardiac sounding chest pain which is then confirmed to be STEMI. It defines diagnosis of STEMI, initial management, and onward care. It does not include management of Non-STEMI cardiac chest pain presentations. For these patients, please refer to the acute coronary syndrome (ACS) guidelines.
This guideline is intended for the use of registered healthcare professionals fulfilling a general role in forward medical locations or in an Emergency Department on deployed operations.
TIME IS CRITICAL
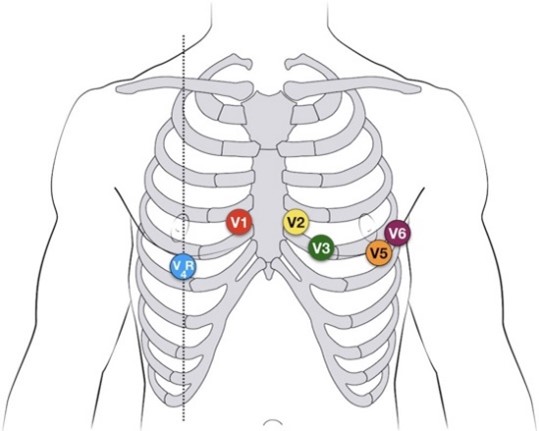
3 Lead ECG AND/OR 12L ECG within 5 mins of presentation – reviewed by clinician
Apply Automated External Defibrillator (AED) Pads
If STEMI confirmed start immediate discussion with Medevac/Aeromed
Assess and Record
Chest pain:
Time:
Symptoms: SOB, sweating, nausea, palpitations
Differential diagnosis to consider (see separate guidelines)
Acute Coronary Syndrome – NSTEMI
Aortic dissection
Inflammatory conditions – Myocarditis/Pericarditis
Pulmonary Embolism
ROLE 1
Immediate treatment – undertake concurrently
Observations: Pulse, BP, Resp rate, Saturations, blood sugar
IV access
Aspirin 300mg PO
GTN spray S/L
Oxygen - if saturations <92%
IV morphine - as required for pain
IV antiemetic - (post opiate and most pts will need when transported)
Ensure continuous cardiac monitoring and availability of defibrillation
Monitor through AED pads if needed
Transfer IMMEDIATELY to R2/3/HNF as able – continuous monitoring while waiting
Thrombolytic agents not available in the role 1 setting
Aeromed – will need consideration for definitive level care UK/Host Nation
Immediate treatment on arrival to Role 2– undertake concurrently
Investigations *as available
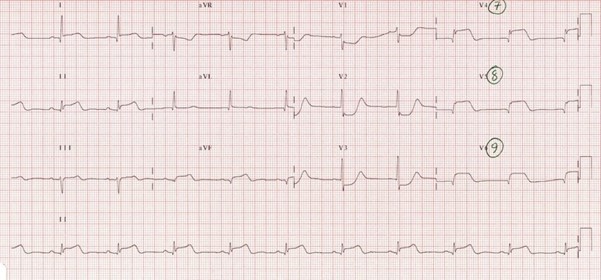
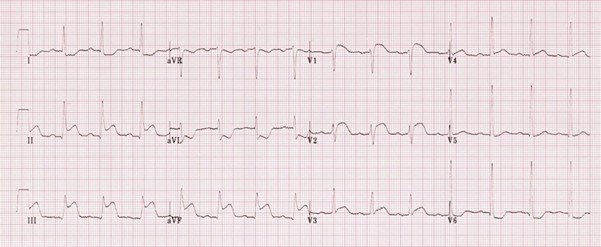
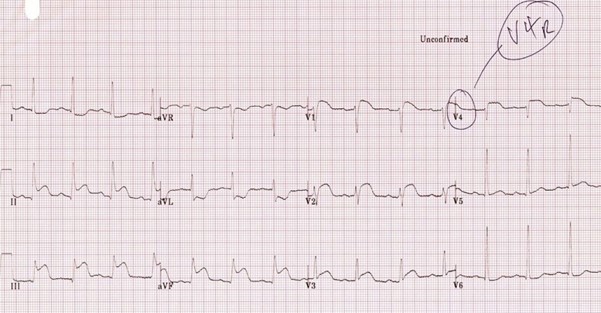
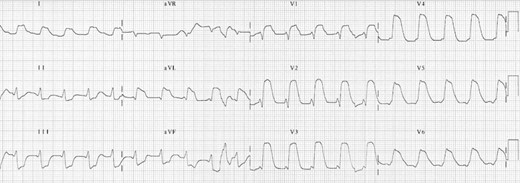
Review ECG and repeat
STEMI NOT Confirmed?
STEMI Confirmed?
Give loading dose of second antiplatelet agent as determined by available formulary (adjust as per thrombolysis guidance if thrombolysis to be given)
Thrombolyse within 12 hours of symptom onset AT LOCATION IF able AND Primary percutaneous coronary intervention (PPCI) not available within 120 minutes - thrombolysis guidelines below
Thrombolysis – For STEMI Only
Tenecteplase is the first-choice thrombolytic agent
Give WITH enoxaparin AND antiplatelets as described below
Contraindications are:
|
Acute Pancreatitis |
GI bleed within 6 months |
|
Aneurysm or Aortic dissection |
GI ulcer within 3 months |
|
AV malformations |
History of oesophageal varices |
|
Bacterial endocarditis |
Major surgery or trauma within 3 months |
|
Bleeding diathesis |
Prolonged or traumatic CPR |
|
Coagulation defects |
Anticoagulant therapy and/or INR > 2.5 |
|
Coma |
Uncontrolled hypertension (systolic > 200mmHg or diastolic > 100mmHg |
|
History of CVA within 6 months |
Pregnancy |
Tenecteplase: IV bolus given over 10 seconds.
|
Patients' body weight category (kg) |
Tenecteplase (U) |
Tenecteplase (mg) |
Corresponding volume of reconstituted solution (ml) |
|
< 60 |
6,000 |
30 |
6 |
|
≥ 60 to < 70 |
7,000 |
35 |
7 |
|
≥ 70 to < 80 |
8,000 |
40 |
8 |
|
≥ 80 to < 90 |
9,000 |
45 |
9 |
|
≥ 90 |
10,000 |
50 |
10 |
Enoxoparin:
Give IV bolus enoxoparin 30mg (Adults 18–74 years, omit if 75 years or over)
Follow with SC injection immediately, which is weight adjusted:
Antiplatlets:
Ensure one off 300mg Aspirin has been given
Give second antiplatelet - Clopidogrel 300mg ideally (omit if patient > 74 years)
Post thrombolysis care:
Ensure patient in critical care area
Repeat ECG after 60 – 90 mins to confirm effectiveness
Successful clinical reperfusion suggested by;
DO NOT REPEAT THROMBOLYSIS
Evacuation
ALL cases of ACS (STEMI and NSTEMI) require evac to a cardiac centre ASAP
Prolonged care
Observe in critical care area with continuous ECG monitoring
Resus equipment must be to hand including defibrillator
Addition medication to include; statin, ACEi, Beta blocker though these are only available in role 3
Smoking cessation if this has been a risk factor
Be wary of those with RV infarct – any drugs that reduce venous return, like nitrates or diuretics, can reduce cardiac output and precipitate shock
When compared with PPCI, thrombolysis treatment for STEMI is associated with a higher likelihood of complications including Myocardial rupture, severe mitral regurgitation and Ventricular septal defect