
Pericarditis
Objectives
To outline the management of patients presenting to deployed medical facilities with suspected pericarditis.
Scope
This guideline intends to cover the initial investigations and management of patients presenting to the deployed medical treatment facilities with suspected and then confirmed acute pericarditis. It confirms the definition of acute pericarditis, sub-acute and chronic pericarditis, management, and onward care. It also covers occupational considerations.
Audience
This guideline is intended for the use of registered healthcare professionals fulfilling a general role in a forward medical locations or in an Emergency Department on deployed operations.
Initial Assessment & Management
Pericarditis- Inflammatory disorder of the pericardium, in the developed world most commonly idiopathic or secondary to recent viral infection. Globally, and in developing countries, tuberculosis (+/- HIV association) is most common cause, especially in endemic regions.
Acute pericarditis - symptoms lasting ≤ 4 weeks
Sub-acute/ incessant pericarditis - symptoms lasting > 4 weeks but < 3months without remission
Chronic pericarditis - symptoms lasting > 3months without remission
Recurrent pericarditis - A recurrence of pericarditis by diagnostic criteria following a symptom-free interval of ≥4 weeks
Diagnosis:
Two of the following criteria-
- Chest pain (>85–90% of cases) - typically sharp and pleuritic, improved by sitting up and leaning forward
- Pericardial friction rub (≤33% of cases) - superficial scratchy or squeaking sound best heard with the diaphragm of the stethoscope over the left sternal border
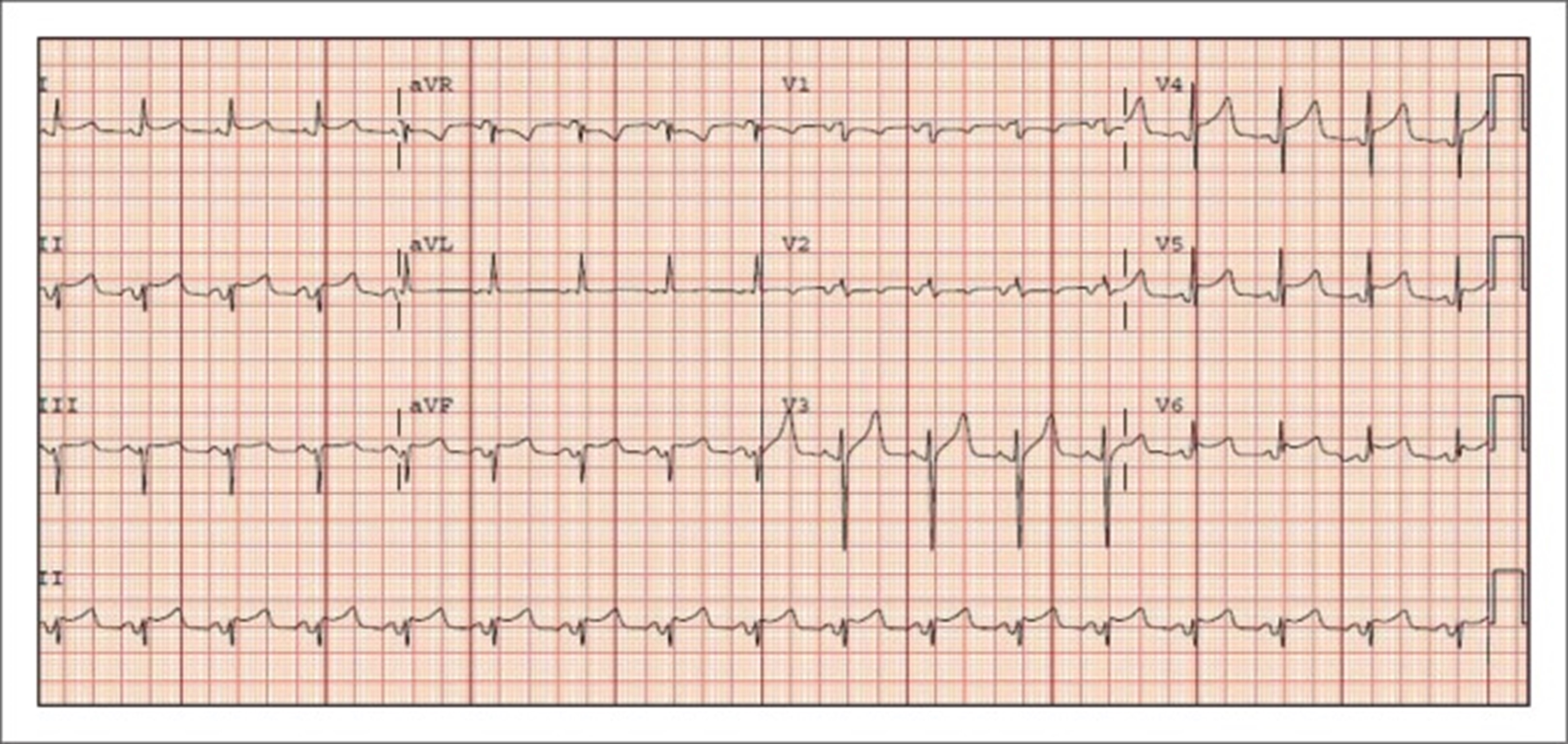
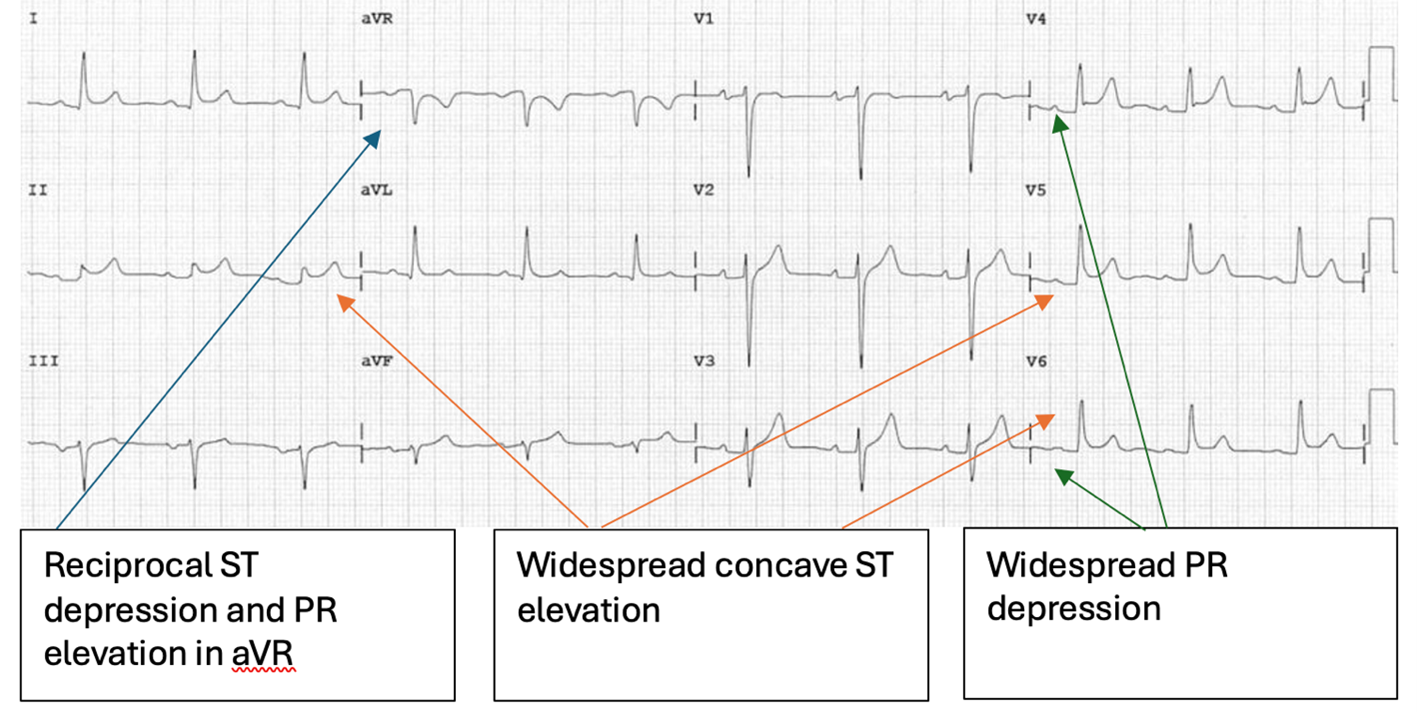
- ECG changes (up to 60% of cases) - new widespread ST elevation or PR depression in the acute phase – see ECG below
- Pericardial effusion (up to 60% of cases, generally mild)
High risk features consider urgent transfer to Role 3 facility-
- Fever >38.0
- Subacute course (symptoms developing over several days or weeks)
- Large pericardial effusion (>20mm)
- Cardiac tamponade (Consider if hypotension, raised JVP, muffled heart sounds)
- Myopericarditis – see myocarditis guidelines
- Failure to respond to NSAID treatment after 7 days
- Immunosuppression
- Trauma
- Oral anticoagulant therapy
Initial Management:
Investigations-
- Observations – HR, BP, O2 saturations
- 12L ECG – classical features vs early repolarisation (see ECGs below)
Stage 2: ST segment elevation and PR depression have resolved and T waves may be normal or flattened
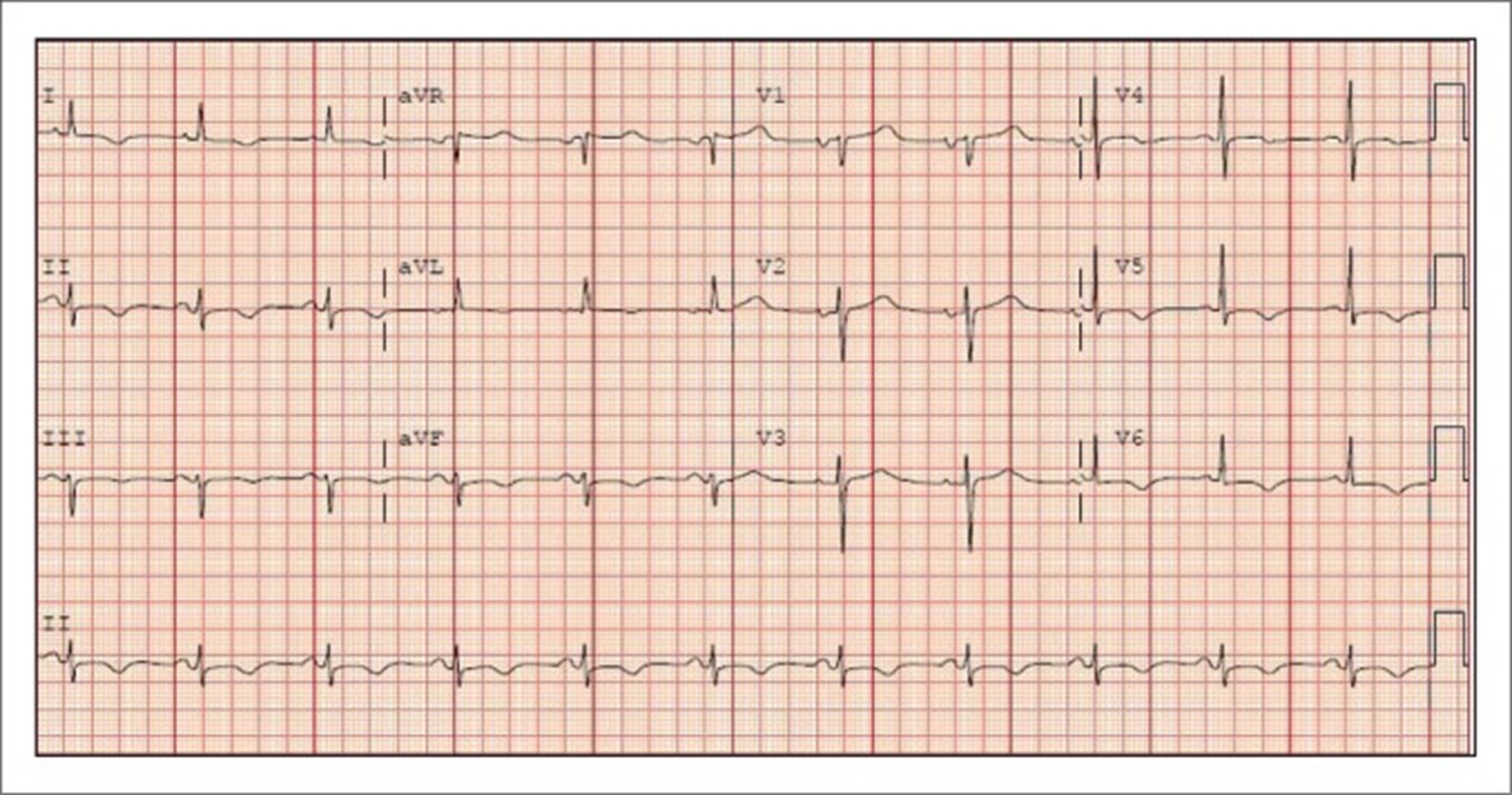
Stage 4: T waves return to the upright position, and ECG normalises

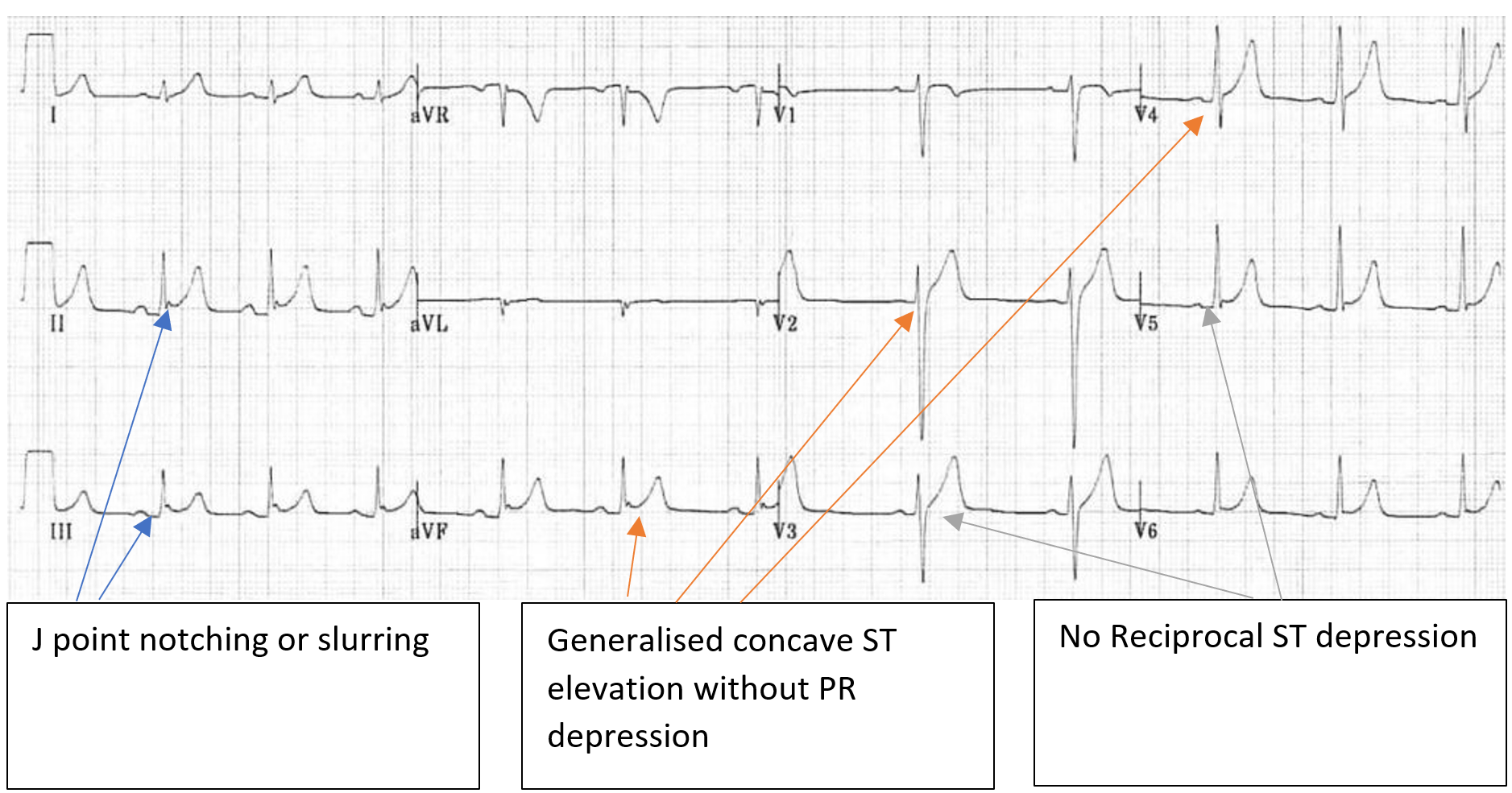
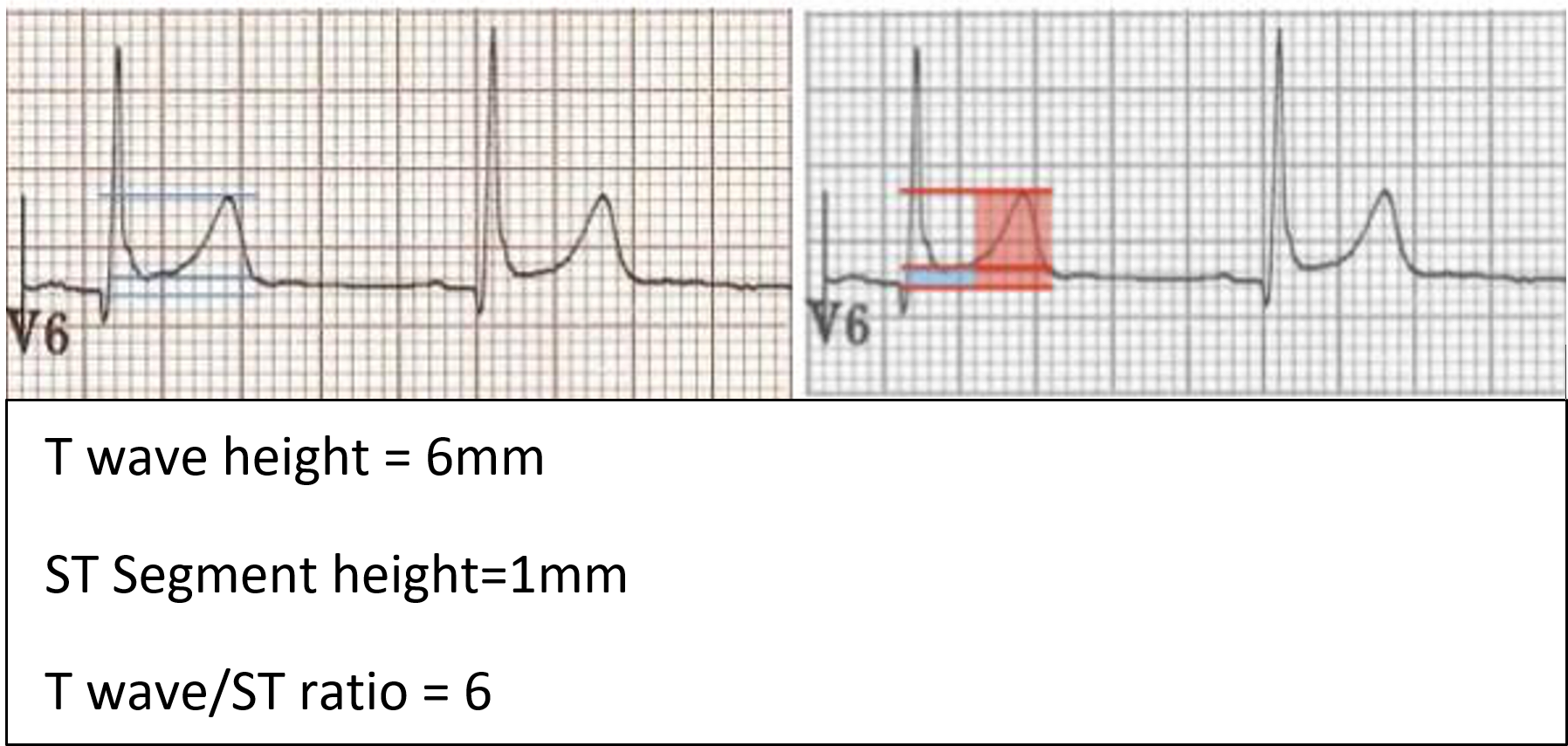
Differences between BER and ECG changes of pericarditis:
- ST elevation limited to precordial leads
- No PR depression
- Prominent T waves
- Ratio of T wave amplitude to ST elevation should be >4 if BER is present (the T wave in BER is normally 4 times the amplitude of the ST segment elevation, ie. ST segment elevation is less than 25% of the T wave amplitude in BER)
- ST segment elevation in BER resolved when the person exercise
- Notched J point elevation, AKA ‘fish hook’ pattern, best seen in lead V4
Treatment
Treatment consists of anti-inflammatories. There is no significant difference between the ibuprofen and aspirin in the ranges described below. At present Colchicine is not carried in deployed modules, but is a valuable part of sustained treatment, reducing recurrence by 40%. As such it should be commenced when possible, either locally sourced or on return to firm base.
- Ibuprofen/ Aspirin + Colchicine as outlined below. In cases with high-risk features consider a longer tapering course of anti-inflammatory treatment depending on clinical response.
- With all treatment options give gastroprotection with PPIs
- Patients should be re-reviewed after 1 week to assess response to treatment
NB: The very high doses suggested in the Aspirin box are correct for aspirin as an anti-inflammatory rather than in its more commonly encountered antiplatelet role which will be an order of magnitude lower.
If pain/CRP worsen during the tapering phase of pericarditis treatment, return to the last effective dose and taper more slowly.
|
Drug |
Dose |
Treatment duration |
Tapering regime: reduce total daily dose by... |
|
Ibuprofen |
600mg – 800mg TDS |
1-2 weeks |
~ 200-400mg per week |
|
Aspirin |
750mg - 1000mg TDS |
1-2 weeks |
~ 250-500mg per week |
|
Colchicine |
500 micrograms once daily (<70kg) or twice daily (>70kg) for 3 months |
3 months |
N/A |
Advanced Assessment & Management
Advanced Investigations
- Chest x-ray
- FBC, U+Es, CRP
- Cardiac enzymes to differentiate from Myocarditis (as available)
- POCUS - Focused Echo to assess for pericardial effusion (if available)
Advanced Treatment
- Significant complications of acute pericarditis are rare.
- Large pericardial effusion and tamponade MUST be excluded at first presentation.
- Cardiac Tamponade is a medical emergency and should be treated as such
- Cardiac instability would not be expected and if present suggests alternative diagnosis e.g STEMI or myocarditis – see appropriate guidelines
Prolonged Casualty Care
In cases with high-risk features consider a longer tapering course of anti-inflammatory treatment depending on clinical response.
Exercise restriction:
In uncomplicated pericarditis physical activity should be restricted while there features of active disease (i.e. ongoing symptoms, raised CRP, still receiving aspirin/ ibuprofen therapy). Following this, and after MO review, there should be a gradual phased return to exercise (but not before 3 months) under the direction of a PTI. Given need for exercise restriction, likely all patients will require evacuation from theatre.
Follow up:
Service personnel with pericarditis complicated by any of the above high-risk features should be referred to a service cardiologist before returning to exercise