
COPD
Warning
Objectives
To outline the expected management of COPD in the operational environment
Scope
This Guideline covers diagnosis and management in Role 1-3 settings including intensive care of adults with COPD.
This guideline covers clinical diagnosis, assessment of severity, management (initial and prolonged), and differential diagnosis of COPD exacerbations.
Audience
This guideline is intended for use by registered healthcare professionals fulfilling a general role in forward medical locations or in an emergency department in a deployed hospital setting
Initial Assessment & Management
Background
COPD is a respiratory condition which may present in the deployed setting as a poorly controlled chronic condition, or as an acute exacerbation characterised by obstructive lung pathology. Treatment is aimed at reversing the underlying cause and managing symptoms.
All patients with COPD should be known to primary care and followed up as part of chronic diseases monitoring on an annual basis.
COPD is uncommon in the military age population with symptoms typically beginning in the 5th decade of life. It may present in older serving personnel, contractors, and entitled civilians.
Diagnosis
Suspect COPD in patients over 35 years old with one or more risk factors and symptoms. Risk factors include Smoking or a range of occupational and environmental exposures including to Coal dust, grains, Silica, Certain fumes or chemicals (such as welding fumes, isocyanates, and polycyclic aromatic hydrocarbons) and Air pollution.
| Symptoms | Signs |
| Breathlessness — typically persistent, progressive over time, and worse on exertion | Examination may be normal |
| Chronic/recurrent cough | Increased respiratory rate |
| Regular sputum production | Hyperinflation of the chest |
| Frequent lower respiratory tract infections | Accessory muscle use & pursed lip breathing |
| Wheeze | Wheeze and/or crackles |
Whilst not possible in the deployed setting, definitive diagnosis is made based on post bronchodilator obstructive pathology on spirometry with an FEV1/FVC ratio less than 0.7 as well as symptoms suggestive of COPD. Significant limitation and potential for exacerbation may exist in patients who do not fulfil these criteria, particularly if there is on-going exposure to cigarette smoking.
Initial assessment and management
An acute exacerbation of COPD occurs when there is a sustained worsening of symptoms with rapid onset requiring medical treatment.
Common causes for exacerbations:
- Infection
- Most commonly viral but also bacterial infections
- Exposure to environmental pollutants.
Signs and symptoms of an acute exacerbation include increased cough or breathlessness, increased sputum production or a change in its colour or consistency, an expiratory wheeze, fever, and tachycardia.
Differential diagnosis:
- Pneumonia
- Pulmonary Embolism
- Pneumothorax secondary to bullous rupture in patients with COPD (note large intact bullae may mimic pneumothorax on examination)
- Acute heart failure
- Cardiac ischaemia
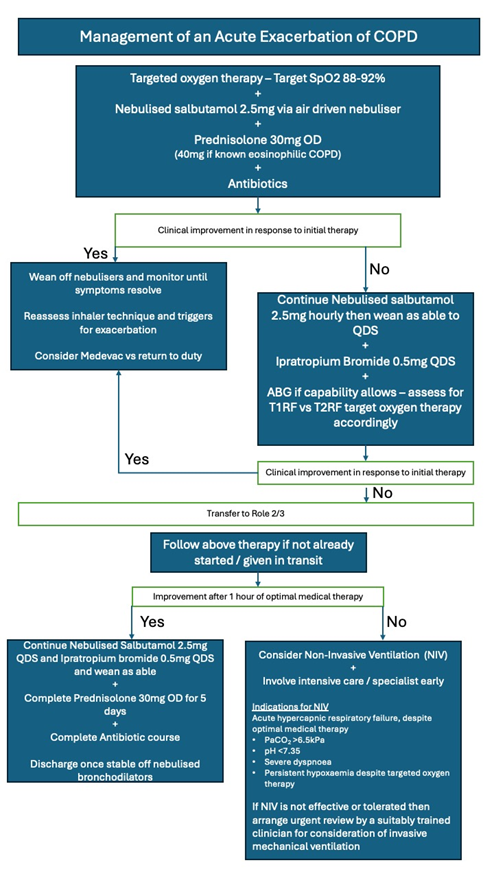
Management
Targeted oxygen therapy. with widespread lung disease, excess oxygen risks causing a shunt, leading to dangerous accumulation of CO2. A venturi mask allows for a known percentage of oxygen to be delivered so these are preferred to deliver a target SpO2 of 88-92%. Nasal cannulae at 1-2L can be used in lieu of a 24% venturi.
Short acting beta-2 agonist (Salbutamol) Give 2.5mg Salbutamol via an air driven nebuliser. Oxygen driven nebuliser may cause a shunt to develop and dangerous accumulation of CO2.
- If an air driven nebuliser is not available, then salbutamol 100mcg inhaler can be given via a spacer every 60 seconds up to 10 puffs.
- Give hourly initially but reduce to QDS once stabilised and wean off as able.
Add ipratropium Bromide 0.5mg via an air driven nebuliser if the initial salbutamol dose was ineffective. Continue QDS. Wean off once improving.
Give prednisolone 30mg OD (If oral medication is not tolerated e.g vomiting then give Hydrocortisone IV 100mg QDS). Continue until symptoms have improved (or minimum 5 days). Give Prednisolone 40mg OD if patient has known eosinophilia.
Antibiotics as per deployed antibiotic guidelines considering allergies. If the patient is known to have a history of pseudomonal infection – then add anti-pseudomonal cover, ideally due to known sensitivities, or if empirical, after failure of first line antibiotics.
If available at this role, take an Arterial blood gas sample for PaO2, PaCO2, and pH.
If a patient has CPAP for sleep apnoea – this should be used whilst sleeping.
Medevac to Role 2/3 for patients not responding to nebulised treatments.
Monitor with an ECG if tachycardiac, for atrial arrhythmias and myocardial ischaemia.
Stop long-acting maintenance muscarinic antagonists (e.g. Glycopyrronium, tiotropium, umeclidinium) to avoid overdose while ipratropium bromide is given. This includes combination (LABA/LAMA/ICS) inhalers e.g Trelegy
Continue maintenance long-acting beta-2 agonist alongside the additional short-acting beta-2 agonist.
Restart regular inhalers once the patient has stopped nebulised ipratropium bromide.
Advanced Assessment & Management
Manage as per Role 1 but with the addition of the following initial measures and escalation as per available resources.
- Early ABG to guide targeted oxygen therapy:
- Type 1 respiratory failure – Hypoxaemia with normal PaCO2
- Target SpO2 94-98% unless directed by a specialist
- Type 2 Respiratory failure – Hypoxaemia PLUS PaCO2 >6.5kPa
- Target SpO2 88-92% unless directed by a specialist
- Type 1 respiratory failure – Hypoxaemia with normal PaCO2
- CXR
- ECG
- Bloods inc FBC (if high eosinophils -->40mg prednisolone rather than 30mg)
- Sputum and blood culture to guide antibiotic therapy
If they have hypercapnic respiratory failure that persists after optimal management for 1 hour, the following criteria are used to commence NIV:
Indications for NIV
- PaCO2 >6.5kPa
- pH <7.35
- Severe dyspnoea
- Persistent hypoxaemia despite targeted oxygen therapy
Contraindications to NIV
- Absolute
- Undrained pneumothorax
- Facial Burns
- Fixed upper airway obstruction
- Relative
- pH <7.15, GCS <8 – consider invasive mechanical ventilation
- Vomiting
- Confusion / agitation
NIV Should only be started by suitably trained medical staff in a designated setting. Initiate within 60 minutes of an ABG showing NIV is indicated. An ABG should be repeated within 30-60 minutes of starting NIV.
To deliver effective NIV, the mask must fit well and be tolerated by the patient. An experienced clinician should set initial values for NIV and titrate according to ABG results. The following suggested settings are for guidance only:
- Spontaneous/Timed mode
- IPAP 10-16 – increase over 10-30 minutes if required (do not exceed 30cmH2O)
- EPAP 4 (do not exceed 8cmH2O)
- I:E Ratio of 1:2 or 1:3
- Inspiratory time 0.8-1.2 seconds
- FiO2 to required level for degree of hypoxia after adjusting EPAP
- Ensure a backup respiratory rate is set at 12-16bpm
If there is no improvement despite NIV, or if pH <7.15 and GCS<8, invasive mechanical ventilation may be required. Escalate to ITU
Indications for ITU admission
- Severe dyspnoea with a poor response to initial emergency therapy
- Changes in mental status
- Persistent or worsening hypoxaemia (PaO2 < 5.3 kPa) and/or severe or worsening respiratory acidosis (pH <7.25) despite supplemental oxygen and non-invasive ventilation
- Haemodynamic Instability (need for vasopressors)
Principles for IMV in COPD are as for asthma.
Whilst thresholds for the intensive care support of patients with COPD have lowered in the civilian setting, with patients responding well to short periods (24-48hrs) of ventilatory support, there remains the potential for a prolonged period of care to be required, the suitability of which in the deployed setting will be determined by available resources, including evacuation or repatriation options and own-nation health provision (ie sufficient to support a protracted ventilatory wean).
Prolonged Casualty Care
The patient can be discharged once stable off nebulised treatments. Patients can complete oral steroids and antibiotics away from medical facilities. If a prolonged course of systemic steroids >2 weeks has been required, the steroids should be weaned at 5mg/3days. Ensure regular inhalers are restarted. The patient should be followed up after an exacerbation requiring a hospital admission to ensure treatment is optimal.
Consider triggers and the suitability of a return to an operational environment vs repatriation for optimisation of chronic management.