
Causes of impaired renal function
These are classified into three groups:
- Pre-renal = poor renal perfusion (best sign: hypotension especially if this is postural)
- Renal = nephritis (best sign: urinary dipsticks show blood, protein or both)
- Post-renal = obstruction (best sign: obstruction on ultrasound).
Indications for renal replacement therapy(haemofiltration, dialysis etc)
- There are four indications for renal replacement in the presence of severe AKI.
- Fluid overload (pulmonary oedema)
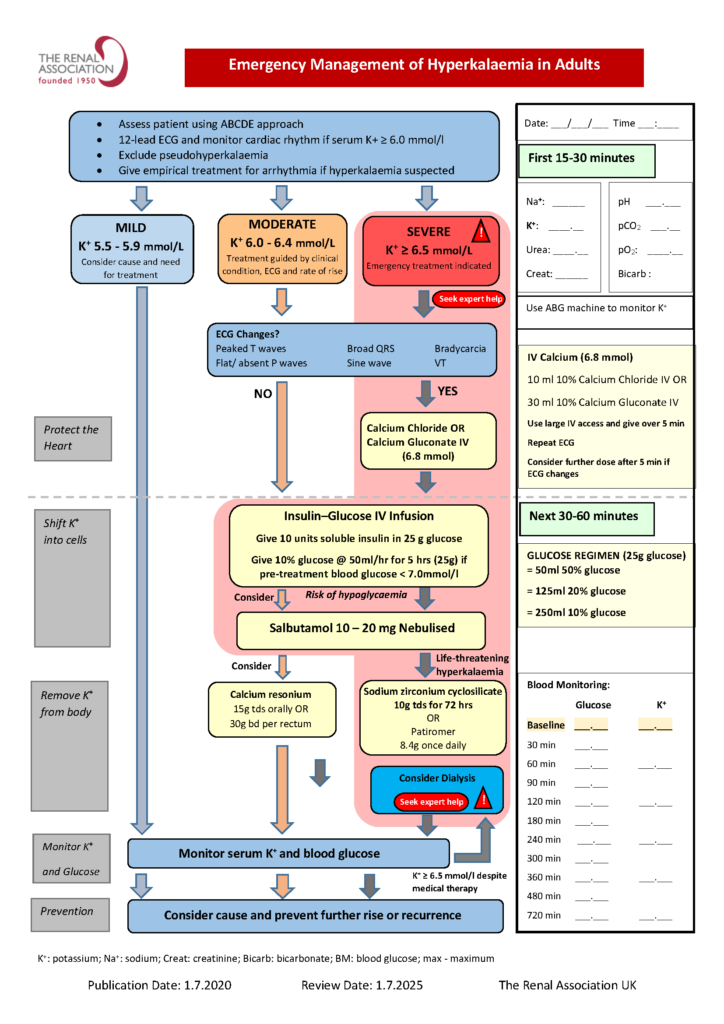
- Hyperkalaemia ([K+]>6.5mmol/l)
- Urea>40mmol/l
- Metabolic acidosis ([HCO3-]<12mmol/l).
Diagnosis and treatment of oliguric AKI
Most causes are medical, usually due to reduced renal perfusion following hypotension (secondary to absolute or relative hypovolaemia), but nephritis is a possibility.
Normal urine output is about 1500mls/24hrs = 60ml/hr
AKI = 400ml/24hrs = 18.5ml/hr
- Hourly urine output; renal function tests (especially serum creatinine) should be monitored regularly in seriously ill patients as soon as medical assessment commences, especially in patients who have suffered trauma, burns or infection who are at particular risk.
- Treat the underlying cause and prevent ongoing injury.
