Heat Illness
Warning
Objectives
To describe the assessment and management of heat illness in the deployed setting.
Scope
This guideline provides a framework for the early assessment and management of patients suffering from suspected or confirmed heat illness in the deployed setting. The focus is on exertional heat illness (EHI), the most common cause in Service personnel, although many of the principles described apply to “classical” and drug-induced heat illness.
Audience
This guidance applies to all medical providers involved in the early assessment and management of the potential heat illness. The role of pre-hospital providers in delivering early recognition and cooling is essential.
Initial Assessment & Management
EHI occurs during physical activity when heat production exceeds the body’s ability to dissipate it, leading to an excessive rise in core body temperature (Tc). It encompasses a spectrum of conditions, from mild to severe. Severe EHI (also referred to as exertional heat stroke) has high morbidity and mortality without early rapid cooling. It can occur in any environment (e.g. during arduous activity wearing PPE).
Presentation
Severe EHI is defined by the presence of CNS dysfunction (e.g. confusion, discoordination, unconsciousness) with a raised Tc (typically >40°C). Collapse, hypotension and agitation are common.
Mild EHI presents as the inability to continue physical activity, during exposure to heat stress, without associated CNS dysfunction. Tc is typically 38.5-40 ˚C and recovery is usually expected after 30 mins with effective cooling. Common symptoms include nausea, dizziness, greater than expected breathlessness and feeling uncomfortably hot.
Classical heat illness presents similarly but in the context of exposure to a hot environment with no or minimal exertion. Drug-induced severe heat illness may occur following ingestion of some recreational drugs and may be associated with severe agitation (see CGO for Acute Behavioural Disturbance - link to follow).
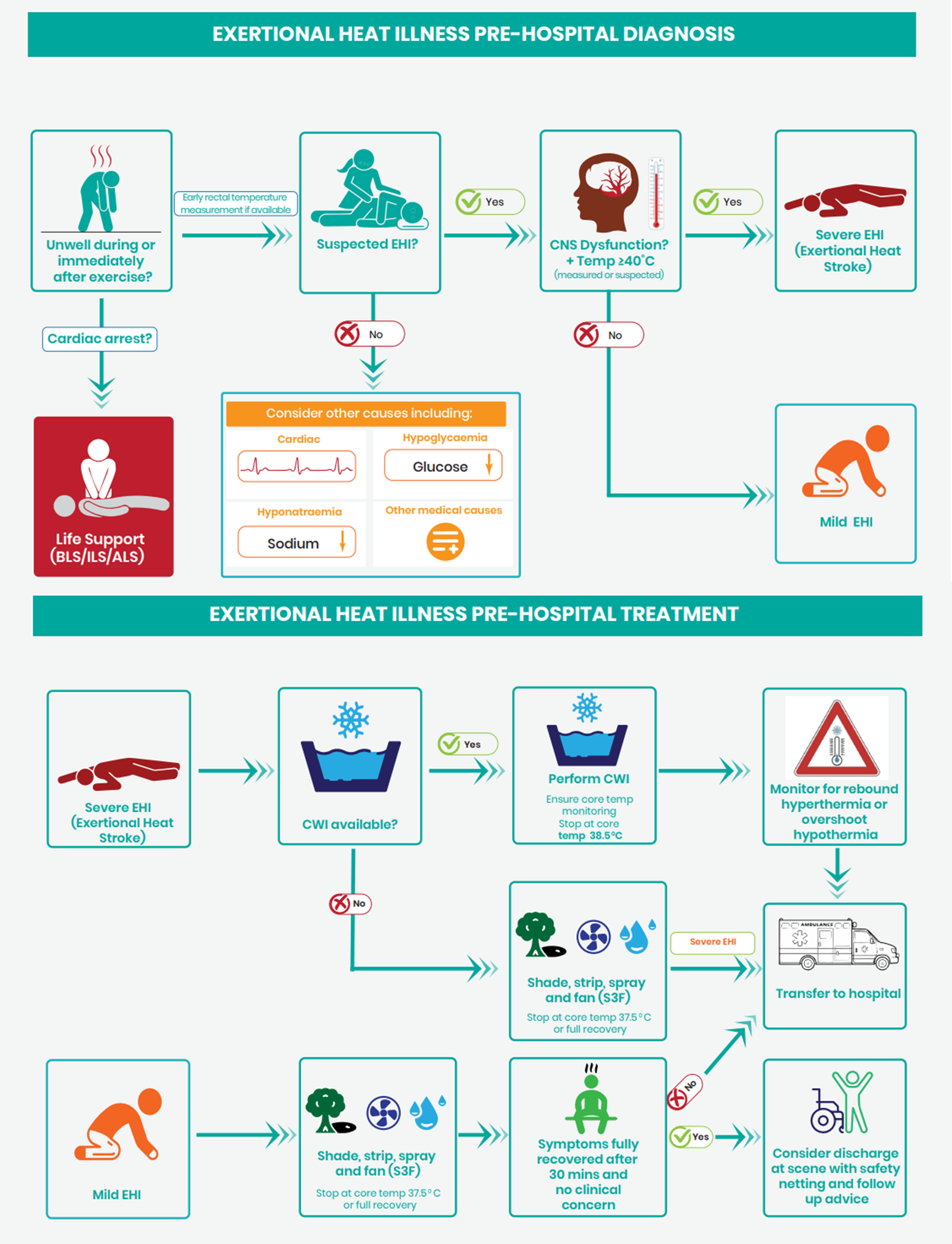
Assessment
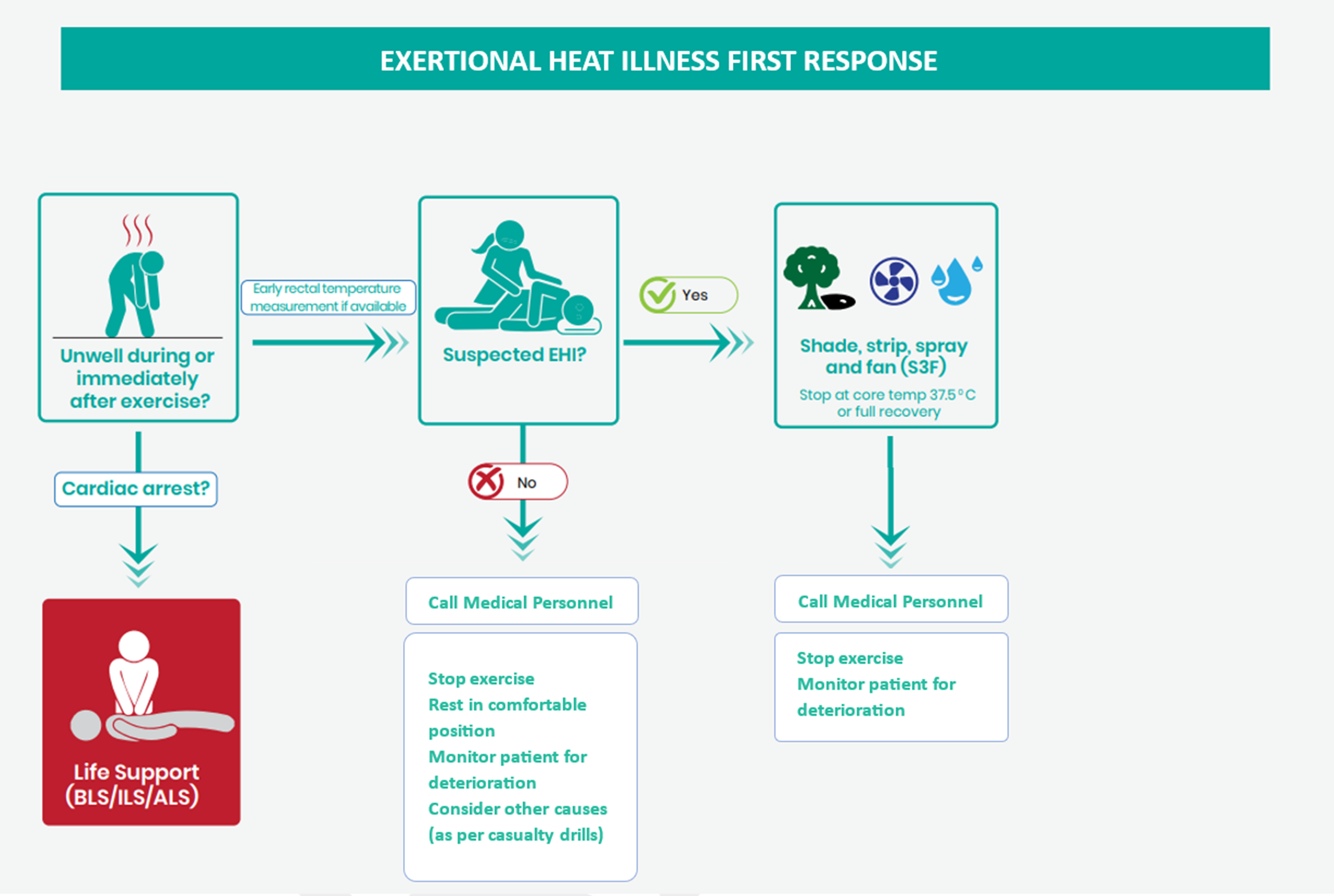
Clinicians must have a high index of suspicion to diagnose Exertional Heat Illness in patients who are unwell during or following exercise. Tympanic thermometers are unreliable in these patients and likely to under-read providing false reassurance. The gold standard for temperature measurement is a flexible rectal temperature probe inserted to 15 cm. If this is unavailable or delayed, then a short (5cm) digital rectal thermometer may be used (a reading >40°C confirms the diagnosis but a reading <40°C does not definitively exclude). If Severe Heat Illness is suspected based on history and presentation but a rectal temperature cannot be performed, the patient should be cooled.
Other conditions that may present with similar signs and symptoms to heat illness include hypoglycaemia, sepsis, hyponatraemia and alcohol intoxication, so these diagnoses should be considered depending on the context.
A rapid MARCH assessment including a rectal temperature should be performed as part of the primary survey. Minimising the time to effective cooling is crucial and only immediately essential resuscitative interventions should take priority. Other interventions can be performed concurrently once cooling has been initiated.
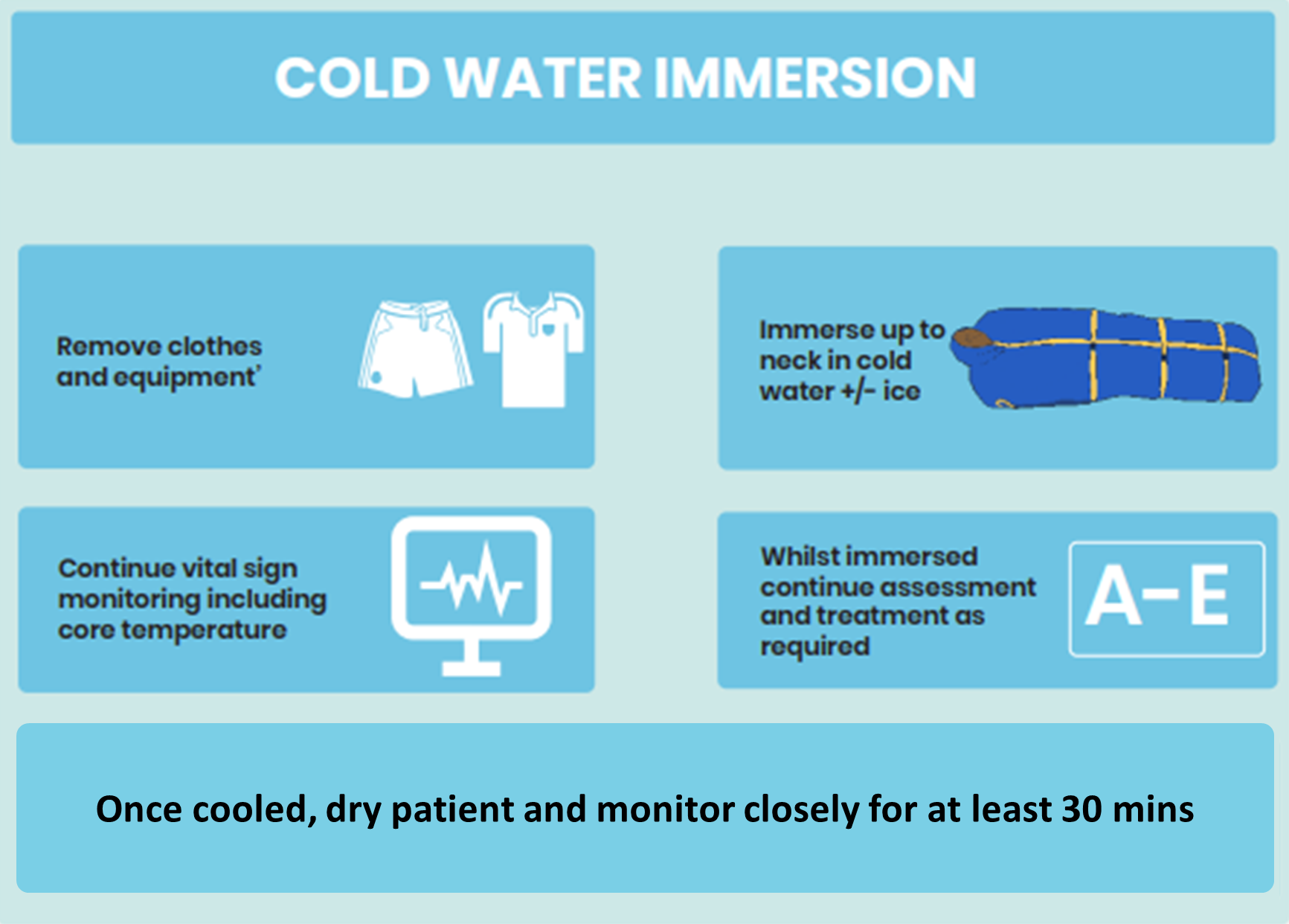
Cooling
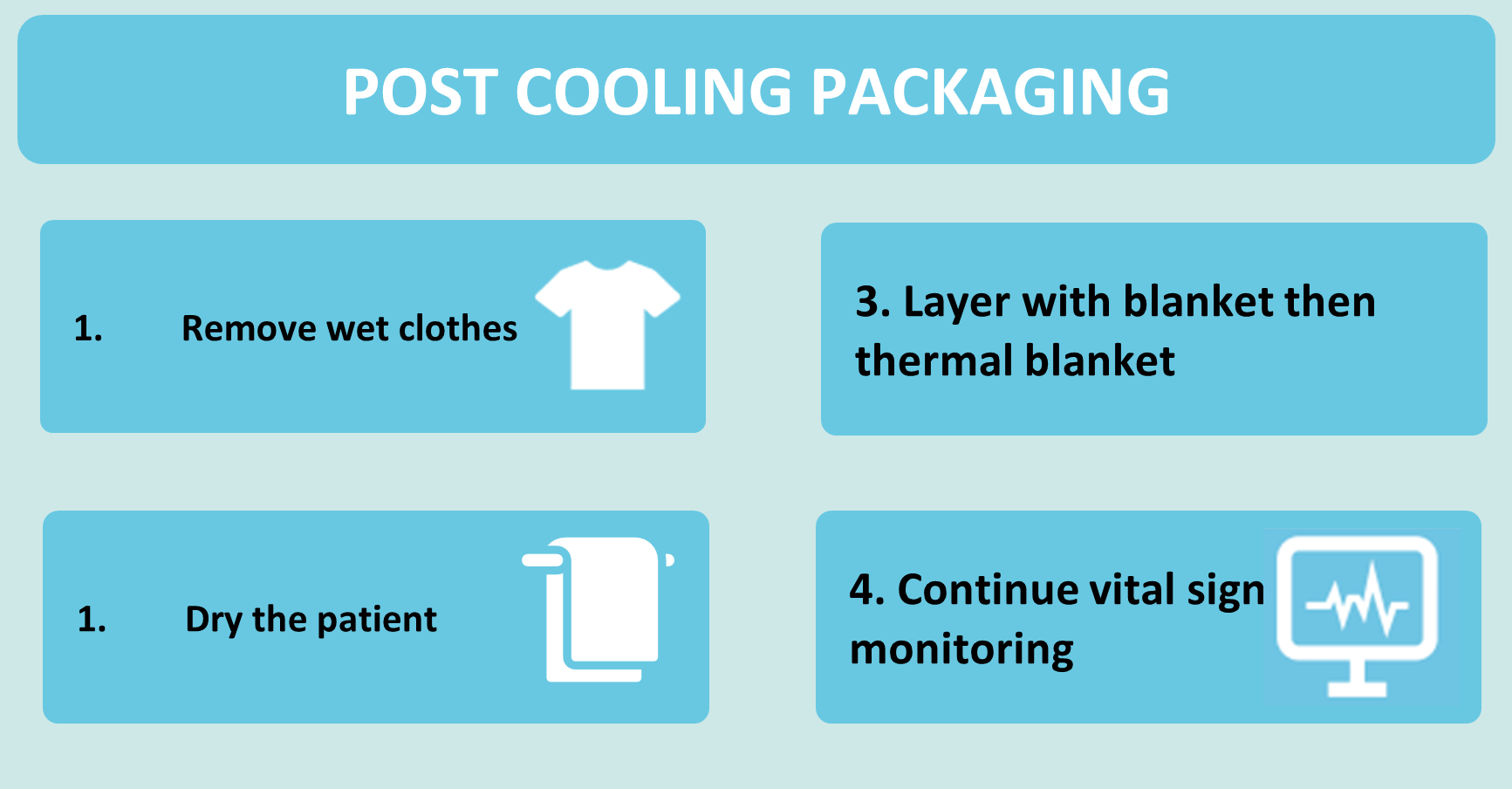
In severe EHI, early rapid cooling is essential. The most effective method of cooling is Cold Water Immersion (CWI). If available, the casualty should be immersed to the upper torso with continuous rectal temperature monitoring. Cooling should continue to a Tc of 38.5°C. Following cessation of CWI, the patient should be dried and wrapped with at least 30 mins ongoing monitoring for potential rebound hyperthermia or overshoot hypothermia.
Cooling during transport is often impractical or ineffective. The routine approach should be to cool first, transport second.
CWI must be used with caution in airway compromise, cardiac arrhythmias with haemodynamic instability and reduced consciousness and is contraindicated in cardiac arrest, as life support takes precedence.
Shade, Strip, Spray, Fan (S3F) is an alternative method of cooling. It should be used in mild EHI or severe EHI when CWI is unavailable or unsafe. The patient should be moved to a shaded area, stripped to their underwear, sprayed with water, and fanned aggressively and continuously. Cooling can be stopped at a Tc of 37.5 ˚C or complete resolution of symptoms.
Patients with “classical” or drug-induced heat illness are also likely to benefit from cooling measures as described above.
Other interventions
Airway - support as necessary (for example in case of reduced conscious level)
Respiration (breathing) - tachypnoea is common and oxygen saturations are often unreliable due to poor peripheral perfusion. Apply high flow oxygen initially if in doubt.
Circulation- tachycardia and hypotension are common. These are expected to improve during/following cooling. Boluses of IV crystalloid fluid may be required to support blood pressure or correct co-existing dehydration.
Head (disability) - blood sugar should be checked and monitored. The conscious level should be regularly re-assessed. Seizures associated with heat illness should be treated following standard protocols for seizure management (including benzodiazepines and airway interventions, if required). Cooling should be continued using the most effective method possible, taking into account the patient condition, personnel and expertise available. If CWI needs to be paused to safely manage a seizure, S3F should continue, with CWI re-initiated once safe to do so.
Advanced Assessment & Management
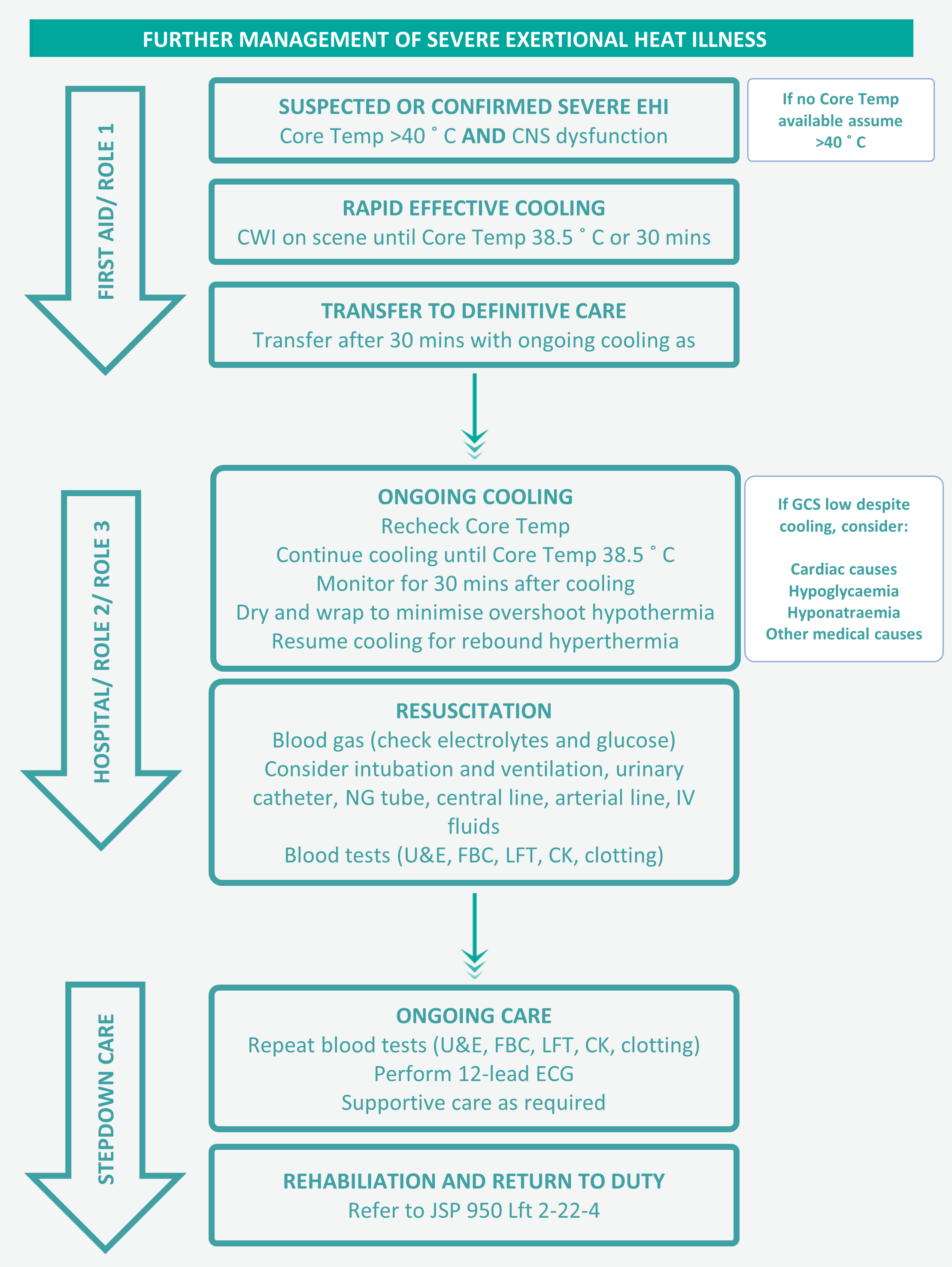
Following immediate management, patients with severe EHI should be urgently transferred to a deployed hospital facility for ongoing care. Patients with mild EHI should be routinely transferred to a primary care facility following immediate management.
The patient should be reassessed, including rechecking the Tc. Clinicians should be aware that pulmonary oedema may develop following severe heat illness, particularly if large volumes of IV fluid have been administered. Resuscitation and supportive care should continue as necessary.
Blood tests should routinely be performed, including U&Es, FBC, LFTs, CK and clotting profile as a minimum. Other tests should be performed as clinically indicated. U&Es, FBC, LFTs and CK should be repeated the following day.
Where impairment to neurological/cardiovascular function is transient and minimal clinical intervention is required, the patient should have a six-hour period of clinical observation. If remaining well, discharge into the supervision of a competent third party may be considered, with clinical review and repeat blood tests at 24 hours. Cases where GCS does not recover rapidly, or where end-organ damage is suspected/proven, necessitate hospitalisation for a minimum of 24 hours.
Potential early complications identified at presentation which are likely to improve within 24 hours of appropriate treatment include metabolic derangement, agitation, respiratory failure and arrythmia. Multi-organ failure may develop in severe cases, particularly if there has been delayed treatment. Occasionally, later complications may arise following cases with a less severe initial presentation.
Patients should be placed on light duties for a minimum of 1 week after confirmed or suspected EHI, including mild EHI. They should not routinely return to full duties prior to blood tests returning to within normal range. JSP 950 Lft 2-22-4 contains full guidance for rehabilitation, specialist review and return to exercise.
Prolonged Casualty Care
Following initial cooling and resuscitation, the principal ongoing management is monitoring and supportive care, including maintaining hydration. In the unlikely event of rebound hyperthermia, S3F should be employed, with CWI initiated if this fails.
Paediatric Considerations
Children with severe Heat Illness should be managed in line with the guidance described above. A small body size is likely to result in more rapid cooling.