
{kind=link}
{kind=link}
Quick reference available here.
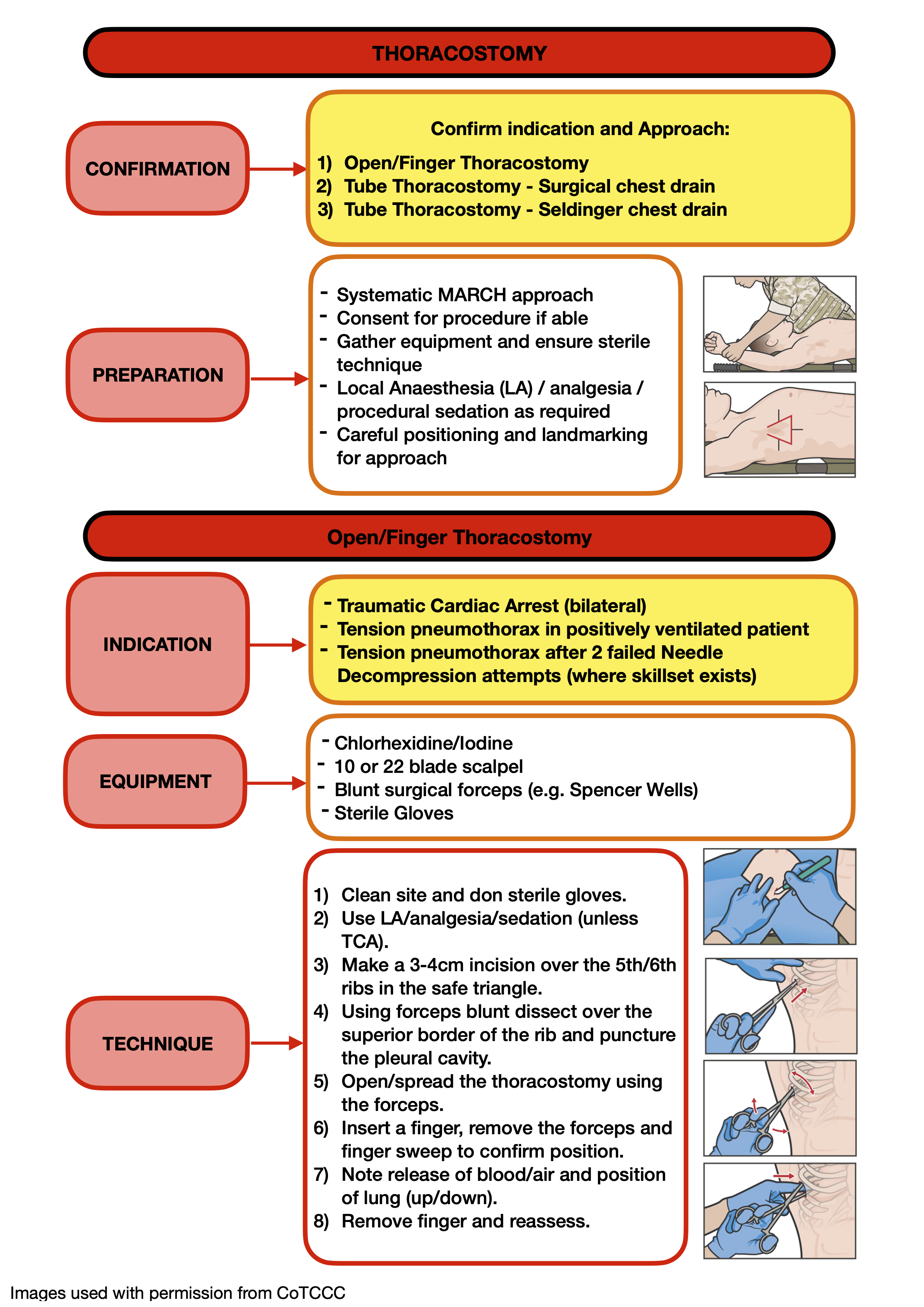
This is an emergent procedure, but time should be allowed to prepare, position the casualty and confirm landmarks as above.
Gather equipment required – Chlorhexidine or iodine to clean site, 10/22 blade scalpel, blunt surgical forceps (e.g. Spencer-Wells), sterile gloves, local anaesthetic and delivery equipment. Clean the surgical site and put on sterile gloves.
This procedure should only be undertaken if the patient is in cardiac arrest or significantly compromised due to a tension pneumothorax, so administering local anaesthetic would not be appropriate, but if the patient is already sedated for positive pressure ventilation then delivering a bolus of analgesia/sedation may be possible and beneficial.
Make a 3-4cm incision into the skin overlying and parallel to the 5th rib.
Using blunt forceps perform a blunt dissection through the soft tissue passing over the superior aspect of the rib. Puncture the parietal pleura in a controlled manner, feeling the “pop” as the forceps tip enters the pleural cavity.
Either spread the forceps repeatedly to open the space OR with closed forceps “strip” the rib space laterally to open a tract through the parietal pleura large enough to admit a gloved finger.
Carefully insert a gloved finger through the incision alongside the forceps and into the pleural space to verify position. Remove the forceps leaving the finger in place. Note any release of air or blood and the position of the lung (collapsed/down or inflated/up) on first insertion. Allow 10-15 seconds of air flow past the finger to decompress the chest cavity.
Remove the finger. In the spontaneously ventilating casualty immediately apply a vented chest seal over the wound. In the positive pressure ventilated casualty leave the thoracostomy open and unobstructed.
Post-Procedure Care
Reassess the casualty for improvement in clinical signs, reduction of respiratory distress or if performed during Traumatic Cardiac Arrest for signs of Return of Spontaneous Circulation (ROSC).
Continue to monitor and record vital signs, provide appropriate analgesia and manage concurrent injuries in line with the MARCH approach. If undertaken forward of the deployed hospital environment, a thoracostomy wound should be considered as potentially contaminated, and prophylactic antibiotics should be administered accordingly, following current antimicrobial guidance.
Return of signs/symptoms of tension pneumothorax suggests thoracostomy obstruction. Every attempt should be made to avoid this by monitoring the site and avoiding physical blockage. If this does occur it will be necessary to “Re-Finger” the thoracostomy. Re-insert a clean gloved finger along the surgical tract into the pleural space and again allow 10-15 seconds of air flow past the finger to decompress the chest cavity. This may be required repeatedly and consideration should be made to surgical chest drain placement in line with the procedure described below.
In the positive pressure ventilated casualty it is not necessary to immediately progress to surgical chest drain placement if there are other clinical priorities but this is likely to be required eventually in nearly all situations to facilitate ongoing care and safe MEDEVAC.
Paediatric Considerations
A smaller incision and smaller forceps may be required in paediatric patients. Careful attention should be paid to passing immediately above the rib in small rib-spaces to avoid the neuro-vascular bundle.
In small children it may be impossible to insert a finger through a rib space. In this situation one or two forcep tips should be used to widen the parietal pleural incision and hold it open for long enough to decompress the pleural cavity.
Prolonged Casualty Care
Continue to monitor vital signs and manage analgesia as per the above recommendations.
Maintain cleanliness of thoracostomy site, consider covering with a vented chest seal to aid with this. Deliver antibiotics in line with current antimicrobial guidance.
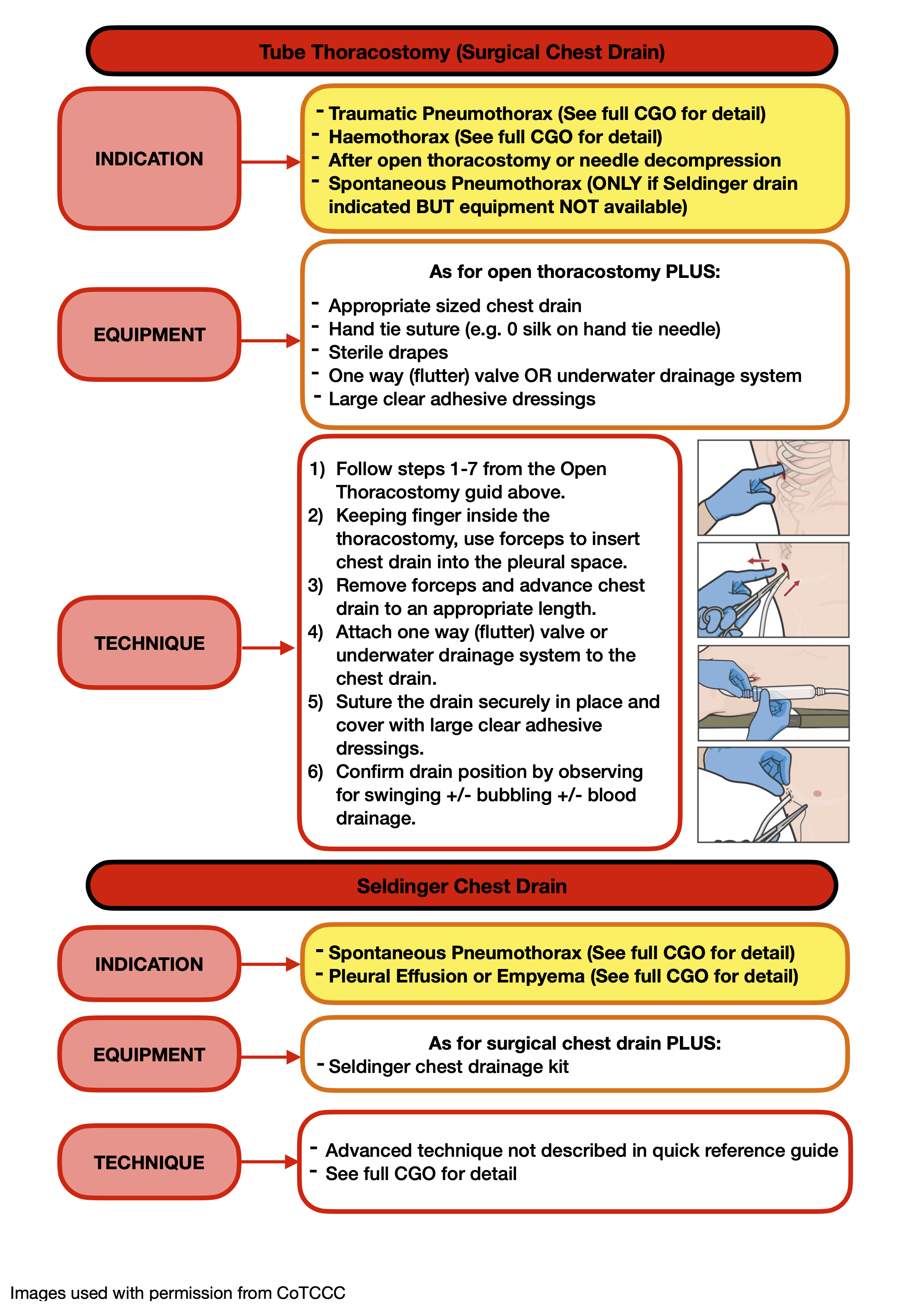
Consider progressing to insertion of a surgical chest drain if the patient experiences repeated episodes of tension pneumothorax requiring re-fingering of the thoracostomy. A drain may also be inserted in preparation for evacuation if it is thought that monitoring or accessing the thoracostomy site may be difficult in transit.