
Needle Thoracocentesis
Objectives
To guide military medical personnel in the management of adult and paediatric patients presenting with a tension pneumothorax.
Scope
This guideline relates to the treatment of adults and children presenting with a tension pneumothorax.
The current devices used by the DMS are the Russell PneumoFix® 8 and the longer Russell PneumoFix® as a rescue device. If PneumoFix® 8 is not available, a 14G cannula can be used as an alternative. Other needle decompression devices (NDDs), for example the ARS, can be used if the user is familiar with its application.
This guideline will refer to PneumoFix® 8 but the landmarks and technique will be common to all devices.
Audience
This guideline is intended for use by registered healthcare professionals fulfilling a general role in forward medical locations or in an emergency department in a deployed hospital setting
Initial Assessment & Management
Needle thoracocentesis Pre-hospital / Role 1 / Role2/3
Indications
1. Suspected tension pneumothorax:
- Usually in the context of penetrating or significant blunt chest trauma
- Spontaneously breathing patients with any combination of worsening hypoxia, worsening respiratory distress, shock, chest pain or chest signs including asymmetry, reduced air entry, hyper-resonance and tracheal deviation.
2. Ventilated patients who develop increasing hypoxia, hypotension and/or increased ventilation pressures where open finger thoracostomy skill set is not available
3. Traumatic cardiac arrest as managed in line with the CGO Traumatic Cardiac Arrest
|
Probable Findings (Spontaneously Breathing Patient) |
Uncommon/Late Findings (Spontaneously Breathing Patient) |
Ventilated Patients |
|
Chest pain |
Hypotension |
Hypoxia |
|
Shortness of breath |
Jugular vein distension |
Hypotension |
|
Respiratory Distress |
Tracheal deviation |
Increasing ventilation pressures |
|
Hypoxia |
Subcutaneous Emphysema |
Decreased air entry |
|
Tachycardia |
Thoracic Hypo expansion |
Jugular vein distension |
|
Decreased air entry |
|
Tracheal deviation |
|
Hyperresonance |
|
Subcutaneous Emphysema |
|
|
|
Thoracic Hypo expansion |
Table 1: Potential signs and symptoms of tension pneumothorax
CAUTIONS
The Pneumofix® (11cm) is longer than the Pneumofix®-8 (8 cm). Pneumofix® should primarily be used as a rescue device in patients where the Pneumofix-8 has failed to reach the pleural space. If this is the case, it is most suitable for use in the 5th ICS, midaxillary line; additional caution must be used to prevent damage to underlying structures.
In third trimester pregnant patients and/or patients with gross obesity, there is an upward displacement of the diaphragm. Therefore, insertion of the NDD should be at the 3rd or 4th intercostal space, mid-axillary line to avoid damage to the abdominal viscera/liver/spleen.
In cold environments the Pneumofix® and Pneumofix® 8 catheters may be stiffer and the potential for lung damage on advancement increases. Additional care should be taken.
Do not insert a NDD through a chest seal.
If insertion through the skin proves difficult do not apply excessive force. If available, use a scalpel to make a small nick in the skin
Incorrect placement may damage surrounding vascular structures. Cardiac tamponade, pulmonary and intercostal bleeding are a risk at the anterior decompression site. Liver, spleen, bowel and cardiac injury are a risk at the lateral decompression site. Monitor for deterioration/bleeding following NDD insertion.
Primary site – 2nd intercostal space, mid clavicular line (2nd ICS MCL)
2nd ICS MCL is the primary needle decompression site in adults. It is accessible and prominent, has a reduced probability of cardiac injury and reduces the chance of blood accumulation in the NDD. See Figure 2 for landmark.
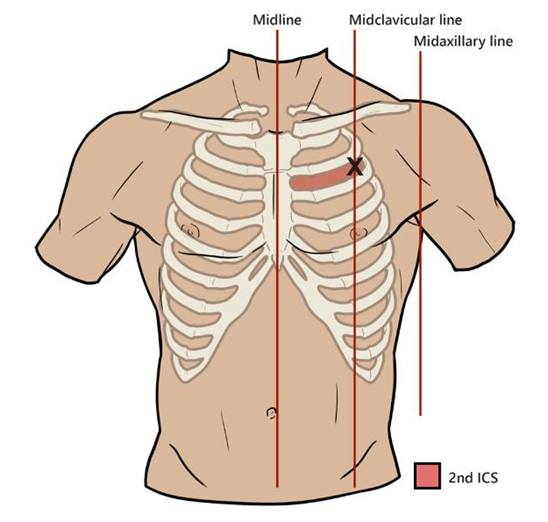
Figure 2: Landmark 2nd ICS MCL
Locate the angle of Louis (foremost bump on the sternum) and palpate laterally on the affected side to locate the 2nd rib. Continue to palpate the 2nd rib laterally and align with the mid clavicular line- this should be in line or lateral to the nipple in most young patients. The second intercostal space is the area located directly below the second rib. NDD insertion is directly above the 3rd rib to avoid the neurovascular bundle.
Secondary site – 5th intercostal space, anterior to the midaxillary line (5th ICS MAL)
Consider needle decompression at the 5th ICS MAL if there is continued failure at the primary decompression site and diagnosis is probable, there is gross chest deformity or there's difficulty accessing the anterior chest wall (entrapment, distressed patient). See Figure 3 for landmark.
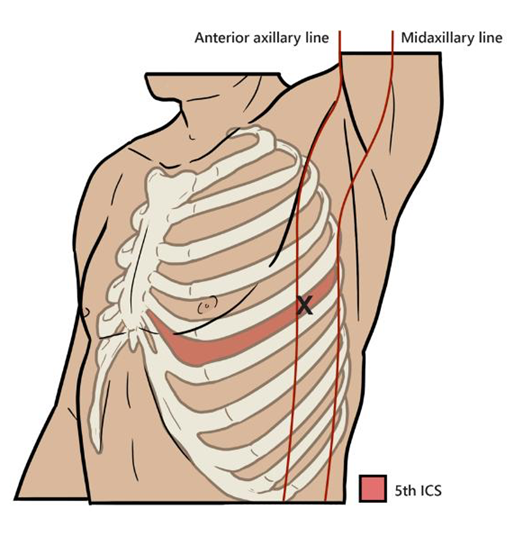
Figure 3: Landmark 5th ICS MAL
Locate the angle of Louis and the 2nd rib on the anterior chest. Count down to the 5th rib and follow the rib laterally to the middle of the arm pit (axilla). The 5th IS MAL is slightly anterior to the midaxillary line and NDD insertion is above the 6th rib. Do not rely on the patients “hand under the arm pit” as a crude anatomical reference without also counting the ribs.
Abducting the patients arm to expose the chest wall can facilitate the landmark identification/procedure. This can be achieved by placing the patients palm under their head. Be aware of humeral intraosseous access displacement.
Procedure
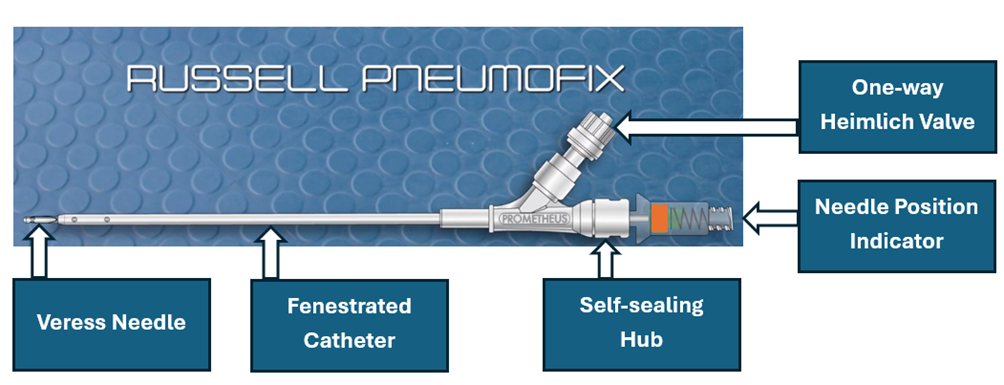
Figure 3: PneumoFix®-8
1. Lift any chest seals placed for open pneumothorax to ensure no accumulation of air due to seal. Replace if no improvement and proceed as below.
2. Clean insertion site.
3. Open the PneumoFix®-8 and confirm the one-way valve is attached.
4. Hold the PneumoFix®-8 hub in a pen like fashion, while supporting the other hand on the chest. Insert the PneumoFix®-8 at a 90-degree angle to the chest, note the orange indicator moving away from the chest.
5. Slowly advance still watching the orange indicator for movement towards the chest.
6. Once the indicator moves towards the chest carefully advance the needle 1cm further.
7. Twist to unlock the needle from the self-sealing hub.
8. Holding the needle in place, advance the catheter a further 2-3 cm over the needle before removing the needle from the self-sealing hub.
9. Dispose of sharps safely.
10. Secure the PneumoFix®-8 to the chest wall using a chest seal or tape. Make sure not to cover the one-way valve port.
11. Reassess the patient for evidence of clinical improvement.
Post thoracocentesis
An audible release of air should not be relied on to confirm correct needle placement.
Observe for an improvement of vital signs, such as SpO2, respiration rate and hypotension (especially if patient is ventilated), and resolution of dyspnoea to confirm correct needle placement and diagnosis
Continually reassess for signs of reoccurring tension pathology.
If there is no observable improvement, reassess for signs and symptoms of a tension pneumothorax. Consider differential diagnosis of shock pathology.
If the suspected diagnosis of tension pneumothorax remains. Insert a second Pneumofix® 8 lateral to the first. Consider an alternative landmark.
Document all procedures, including indications, complications and patient response and initiate immediate evacuation to surgical facility.
Advanced Assessment & Management
Reliance on clinical findings supersedes imaging due to the life-threatening nature of the condition
In the absence of typical symptoms, ultrasound can provide rapid information that may assist in detecting an expanding pneumothorax before tension develops
Absent lung sliding and the presence of a lung point on ultrasound are strong indications of a pneumothorax. Combined with barcode sign, absent lung pulses and/or absence of vertical artifact a pneumothorax diagnosis is compelling
A negative ultrasound does not rule out a tension pneumothorax
Consider ultrasound-guided needle decompression in patients at high risk of developing a tension pneumothorax prior to CAS/MEDEVAC especially if there is expected difficult/no access to the chest during transfer.
CXR/CT may be considered for those patients who are stable and presenting with atypical symptoms
Prepare for urgent finger thoracostomy and chest drain post needle decompression (Reference to CGO)
Prolonged Casualty Care
A syringe can be attached to the catheter and a flush administered. However, this is not a routine procedure and should only be consider where a decompression was successful, but patency is in question, resources are limited and there are prolonged extraction times.
Utilise the PneumoFix® bag drainage system if available
Consider finger thoracostomy followed by chest seal application if the procedure is within the scope of practice of the clinician on scene (See thoracostomy CGO)
There is a low risk of infection after needle decompression alone, especially if the procedure is performed with strict aseptic precautions. This risk increases in the prehospital setting. Monitor for infection and administered antibiotics in accordance with CGO (See Antibiotic CGO link)
Stable patients who are considered to have no serious injuries following high-energy chest trauma are at risk of developing serious complications. Ensure close monitoring as delayed tension pneumothorax presentations (6 hours) have been documented
Paediatric Considerations
PneumoFix® 8 is not routinely appropriate for use in paediatric patients, and a cannula should be used preferentially. If no other equipment available, it can be used with caution in larger children and adolescents.
To reduce the risk of injury to the intercostal vessels and intrathoracic structures the following sizes of cannula are recommended. (1)
- Small infants/newborns – 24G (yellow)
- Infants – 22G (blue)
- 5-year-old children (18kg) – 20G (pink)
- 10-year-old children (30kg) – 18G (green)
To avoid an unnecessarily deep needle penetration, puncture should be performed under guidance by aspiration of air via a syringe and needle movement should be immediately stopped after the aspiration of air.
Consider the primary insertion site to be 4th ICS MAL.
Additional care should be taken in small children when advancing the plastic catheter and consideration given to insertion of only 2-3cm
Slight deviation from 90-degree insertion angle significantly increases the risk of injury to vital structures
Due to the proximity of the heart to the insertion site, this is of particular importance on the left hemithorax.