
Aortocaval compression (compression of the inferior vena cava and the aorta by the gravid uterus) usually manifests by the 20th week of gestation. This reduces venous return and cardiac output.
In healthy pregnant patients with preserved intrinsic compensatory mechanisms, the effects of aortocaval compression may be absent or minimal. However, in critically ill or hypotensive patients, aortocaval compression may precipitate cardiac arrest and limit the effectiveness of cardiopulmonary resuscitation.
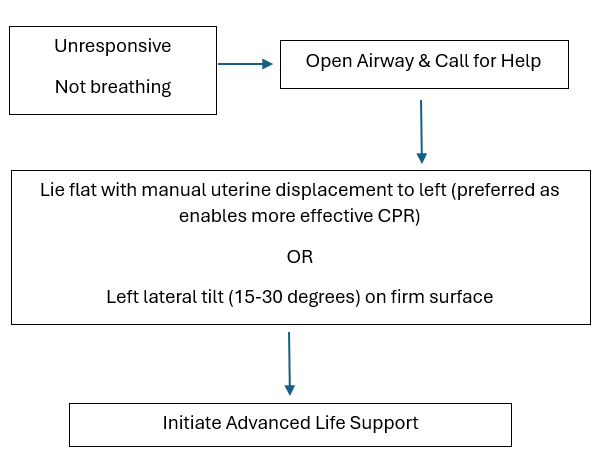
Aortocaval compression can be relieved by manual left uterine displacement or left lateral tilt (although supporting data are derived from non-cardiac arrest and simulation studies).
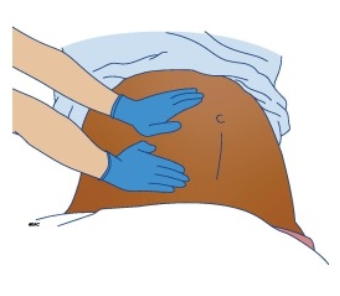
European and UK Resuscitation guidelines suggest performing manual left uterine displacement in maternal cardiac arrest. This can be achieved by placing one or both hands below the uterus, on the patient’s right side, and pushing upwards and to the left. If standing on the patient’s left, reaching across to cup the uterus from below and lifting upward and leftward.



{kind=link}
{kind=link}