Objectives
To guide and support the management of confirmed and suspected hypothermia by military medical personal in all military settings.
Scope
The scope of this CGO is to deliver clinical advice on the recognition and management of hypothermia and to give a framework to decision making in military medical treatment facilities and further forward. This CGO will not cover avalanche rescue.
Audience
This guideline is intended for the use of registered healthcare professionals fulfilling a role in a forward medical location or in an emergency department on deployed operations
Key Definitions and Concepts
Hypothermia is defined as a reduction in core body temperature below 35 degrees. It should be considered a medical emergency.
Core temperature measurement in hypothermia will require a 'low reading thermometer' it is best measured using either a rectal thermometer probe inserted to 15cm or an oesophageal probe in an intubated patient. Aural or skin temperature probes do not give accurate readings at the extremes of temperature.
Recognition of hypothermia can be difficult in the prehospital setting and temperature readings should be considered alongside clinical signs.
Cardiac Arrest or the absence of a palpable central pulse can be difficult to determine in hypothermic patients particularly if the patient has not been removed from the environmental exposure.
Modified Swiss Staging System is the currently used international system for the recognition of hypothermia - see table below.
Note that the Modified Swiss Staging system is only a guide and must be used in conjunction with clinical judgement and additional tests including cardiac monitoring, ECG assessment and point of care blood tests, where available.
| Temperature |
Clinical Findings |
Conscious Level
(AVPU)
|
Risk of Cardiac Arrest |
| Stage I (32-35°C) |
Shivering
Early behavioural changes
|
Alert |
Low |
| Stage II (28-32°C) |
Reduced Consciousness
Absent Shivering
Loss of survival mechanism
|
Responds to voice |
Moderate |
| Stage III (24-28°C) |
Signs of life present
Unconscious
No shivering
Bradycardia, reduced respiratory rate
|
Responds only to pain
or unresponsive
|
High |
| Stage IV (<24°C) |
No signs of life
Cold, stiff
|
Unresponsive |
Hypothermic Cardiac Arrest |
| Stage V (<15°C) |
No signs of life
|
Unresponsive |
Irreversible Death |
Modified Swiss Staging System
Note that temperatures in the above table are for guidance only - if a central temperature cannot be measured then the patient should be assessed clinically.
Initial Assessment & Management
The assessment of the hypothermic casualty will usually start in the pre-hospital space and management of hypothermia should be conducted concurrently with a systematic MARCH assessment. It is crucial that it is considered as early as possible in the assessment.
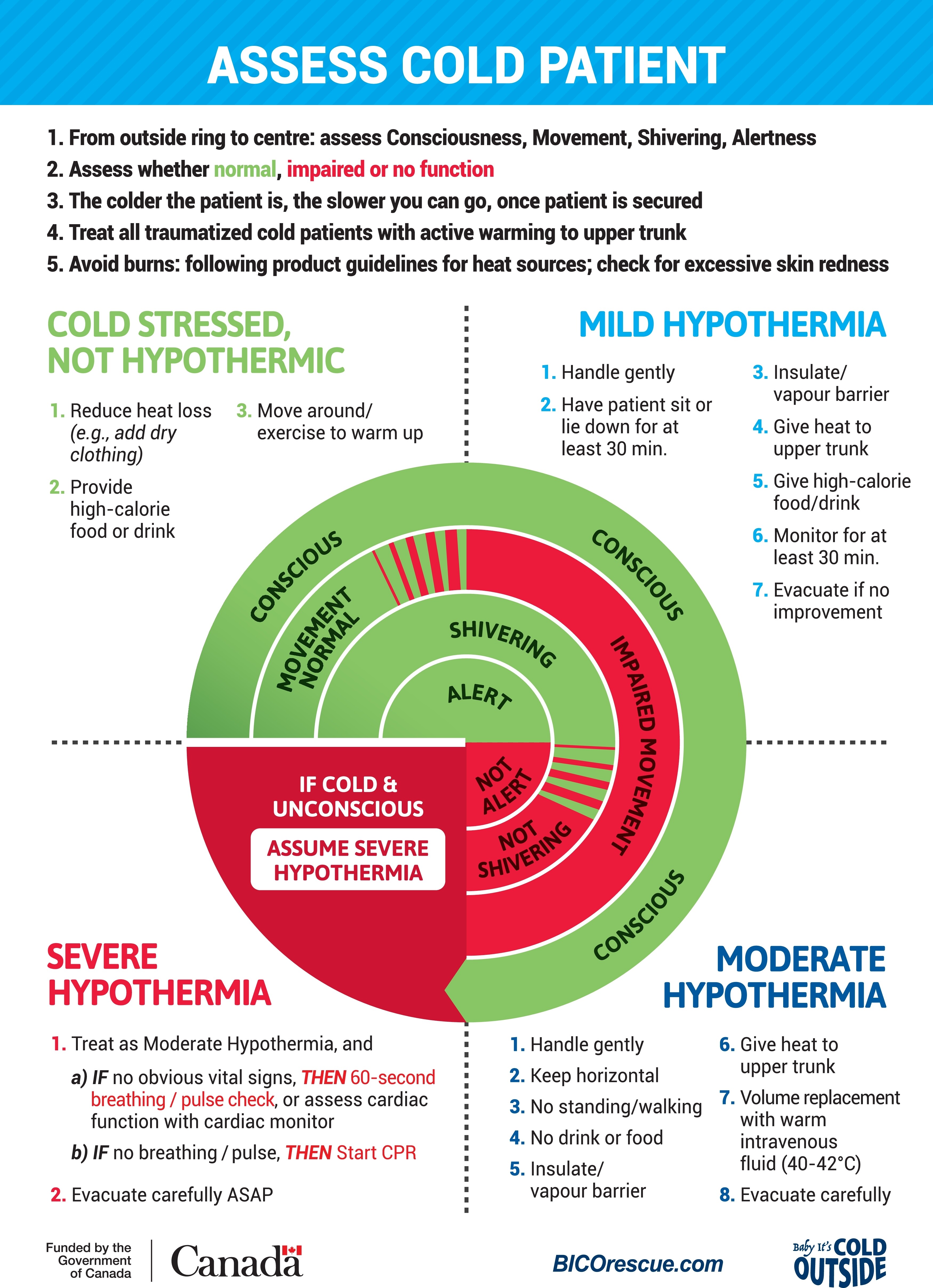
Use the Wilderness Medicine Society Cold Card (see content below or click here for enlarged version) to guide management. In the forward space, accurate core temperature monitoring is unlikely to be possible, so assessment should be symptom-based:
Cold Stressed Patient
Conscious and alert on AVPU scale, moving with normal coordination and shivering.
Not yet hypothermic - reduce heat loss for example by adding dry clothing; encourage movement to warm up, provide high-calorie food or drink.
Mild Hypothermia
Conscious, alert but may become confused, impaired movement likely to be observed, shivering. This correlates with Stage I on the Modified Swiss Staging System.
Monitor for 'umbles': patient may stumble (loss of coordination), fumble (loss of fine motor control), mumble (slurred or slow speech), grumble (behavioural changes) and/or tumble (falling unconscious or inability to stand).
Mild hypothermia - handle gently, if possible sit or lie down; insulate / vapour barrier and give heat to upper torso; provide high-calorie food or drink. Monitor for at least 30 minutes - if no improvement seek to evacuate.
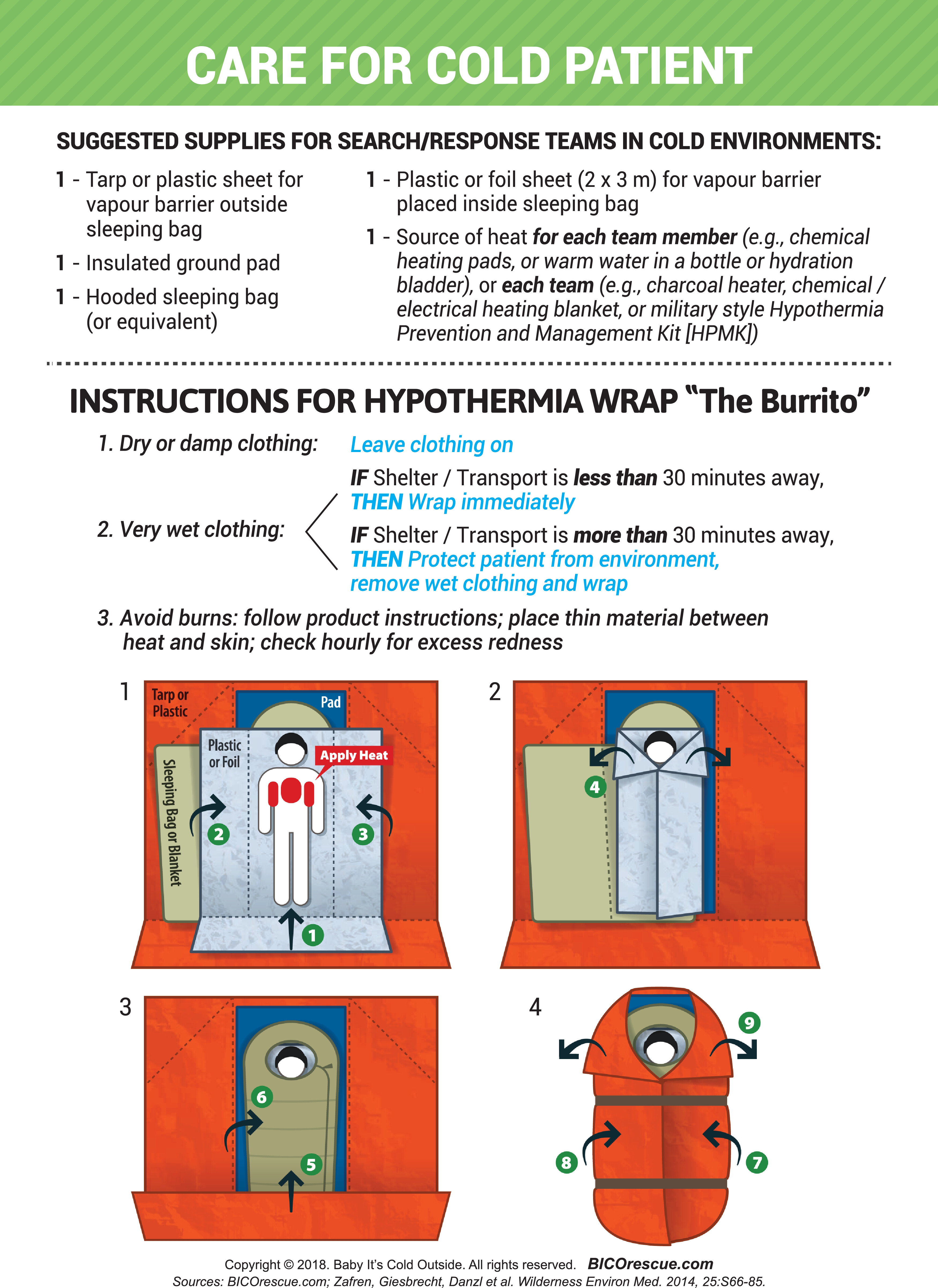
See guidance below on the burrito wrap which provides a solution for optimally packaging a hypothermic patient.
Moderate Hypothermia
Conscious but not alert (V or P on AVPU scale); movement is impaired, patient is not shivering. This correlates with Stage II on the Modified Swiss Staging System.
Moderate hypothermia - handle gently, keep horizontal. Do not attempt to stand/walk patient; do not try to give food or drink. Insulate / vapour barrier and give heat to upper torso; give warm intravenous fluids (40-42°C if possible). Evacuate carefully.
Severe Hypothermia
If the patient is cold and unconscious then assume severe hypothermia. This correlates with Stage III, IV or V on the Modified Swiss Staging System
Treat as for moderate hypothermia above.
If no apparent vital signs - conduct 60 second breathing/pulse check or apply cardiac monitoring. If no breathing/pulse then start basic life support escalating to ALS as soon as a trained provider is available. For ALS, follow the modifications detailed in the accordion content below.
Futility Considerations
The decision not to start CPR on a patient in cardiac arrest may be difficult, but there are circumstances in which death is unfortunately inevitable, for example if there is evidence of unsurvivable trauma such as decapitation or hemicorporectomy. More information is available in the CGO on recognition of life being extinct (ROLE) - link to follow.
Profound hypothermia may offer neuroprotection with the possibility of a good outcome even after a very prolonged resuscitation, but this does not apply if the patient is known to have arrested prior to becoming hypothermic - this means that the patient has not arrested due to cold but has become cold while in cardiac arrest.
If cardiac arrest is believed to have occurred prior to the patient becoming hypothermic then guidance regarding futility in the ROLE CGO should be followed
In addition, resuscitation is futile if the patient's chest is too stiff to allow chest compressions to be delivered.
Advanced Assessment & Management
The initial approach to a suspected hypothermic casualty remains the same in the deployed hospital environment: minimising further heat loss, promoting heat gain and gentle handling are crucial to avoid deterioration and arrhythmias.
The management of cold stress to moderate hypothermia will also not differ significantly apart from the potential availability of better systems to passively rewarm and better access to invasive fluid warming devices.
Management of severe hypothermia will depend on the availability or proximity of extracorporeal life support (ECLS): the gold standard for resuscitation of the hypothermic arrest is via this system and rapid transfer to a facility capable of delivering this should be considered as soon as possible. In severe hypothermia where ECLS is available then the focus should be on maintaining perfusion including use of mechanical CPR if in cardiac arrest. The need to rapidly rewarm in these situations is less important as the hypothermia will reduce cerebral metabolic demand and therefore be neuroprotective.
The use of the HOPE Score is crucial in prognostication prior to the use of ECLS - see content below.
If ECLS is not available, there is limited evidence to support invasive methods of centrally warming a patient, but if a facility is sufficiently equipped to deliver warm fluids and has appropriately skilled and equipped practitioners then the following methods have been described:
- Double bilateral tube thoracostomies, allowing warm fluid to be instilled through one tube and drained through the other.
- Peritoneal lavage with warm fluids.
- Bladder lavage with warm fluids, ideally using a 3-way urinary catheter.
The feasibility of such interventions may be limited by both equipment availability and the ability to provide the large volumes of warm fluid required. Clinicians should factor into decision-making that the evidence of benefit is extremely limited, but in a well-resourced environment then attempting such interventions may be considered worthwhile.