The app and website was publicly released on 2 Apr 2024
Update Jan 2025
The content continues to undergo review by all our cadres.
The content remains subject to the following provisos: - The content will be subject to continuous update and review - Old content (from previous CGOs) will be converted into the new format, using the new tools and layouts - Content may be moved around - The layout will change and reflect the needs of the user - Content will be created - Content may be deleted/retired
CGO development will continue.
Saf [Updated 21 Jan 2025]
Bradyarrhythmia
!Warning
Objectives
To guide the management of patients presenting to medical facilities with bradyarrhythmia.
Scope
This guideline describes the resuscitation of critically unwell patients with bradyarrhythmia. It also considers prolonged casualty care and paediatric circumstances. The management of stable patients without adverse features is also described in brief. Further advice for stable patients should be sought from cardiology experts.
Audience
This guideline is intended for the use of registered healthcare professionals fulfilling a general role in forward medical locations or in an Emergency Department on deployed operations.
Initial Assessment & Management
Bradycardia is defined as a heart rate < 60 beats per minute. Physiological sinus bradycardia is prevalent at rest in deployed personnel due to high levels of fitness and physical conditioning. This is unlikely to be symptomatic.
By contrast, the incidence of symptomatic or pathological bradycardia is likely be low in healthy, pre-screened deployed personnel. However, it may be encountered on operations due to undiagnosed cardiac conditions becoming unmasked, the presence of other unscreened persons working within the theatre of operations (e.g. civilian contractors or allied force personnel) or extrinsic causes e.g. electrolyte imbalance.
Management will be guided by:
Availability of recommended medications in the medical treatment facility
Presence of adverse features
Risk factors for asystole.
In an unresponsive patient, initially follow the Basic Life Support (BLS) algorithm to ensure the presence of a pulse. If there is no palpable pulse CPR should be started, proceeding to the delivery of Advanced Life Support (ALS) as soon as possible.
RCUK Adult Bradycardia 2025
If there is cardiac output and an arrhythmia is suspected:
Assess the patient using the MARCH/ABCD approach.
Correct hypoxia if present
Record a complete set of observations and establish cardiac monitoring
Perform a 12 lead ECG as soon as possible
Obtain IV access
Consider other reversible causes (e.g. presence of electrolyte abnormalities)
Assess for adverse features:
Shock (systolic BP <90mmHg)
Syncope (including recent collapse or transient loss of consciousness without other explanation)
Myocardial ischaemia (cardiac chest pain or evidence of ischaemia on ECG)
In addition, extremes of heart rate (<40 beats per minute) are often tolerated poorly.
If there are no adverse features, assess for the risk of asystole using the following checklist:
Recent asystole
Mobitz II AV block (see accordion content)
Complete heart block with broad QRS (see accordion content)
Ventricular pause > 3s (on a standard ECG at 25mm/sec, 5 large squares = 1 second)
If the patient is stable, additional historical factors include:
Risk of electrolyte disturbance – medications, concurrent illness e.g. diarrhoea/vomiting
Past history of syncope, presyncope, chest pain, breathlessness or oedema
Family history of cardiac arrhythmia, unexplained sudden death or sudden cardiac death
Drug history and allergies
No adverse features or risk of asystole
The patient can be observed.
Adverse features
Apply defibrillation pads pre-emptively. If cardiac output is lost, commence ALS.
Administer atropine 500mcg IV/IO and assess response (targeting a HR >60bpm and improvement in adverse features)
If response is unsatisfactory this can be repeated up to a maximum of 3 milligrams.
No adverse features but risk of asystole present
Use interim measures depending on clinical risk assessment.
Treatment options are dependent on medication and equipment availability in forward medical environments. Continuous vital signs monitoring is required (if available).
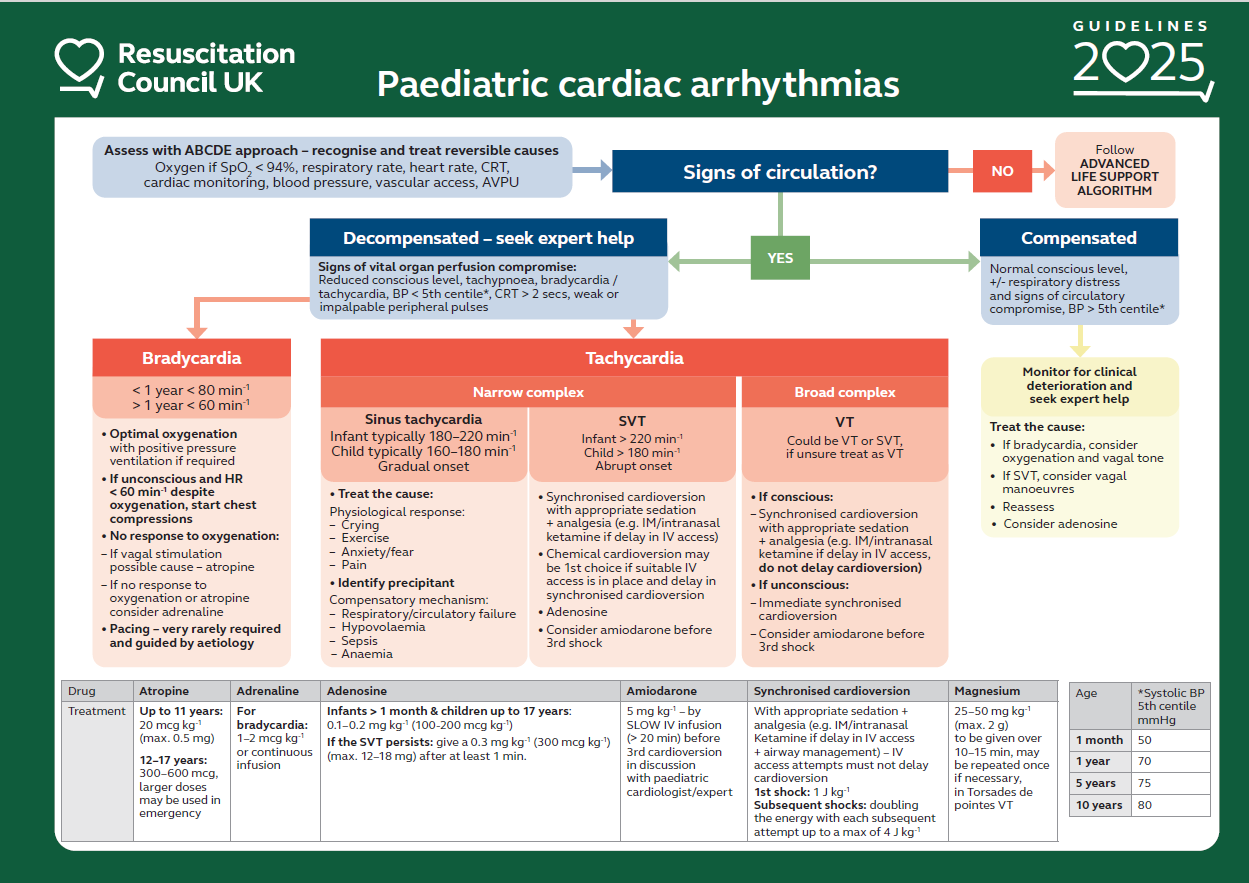
In paediatric bradycardia, consider oxygenation and vagal tone.
If there is evidence of cardiac output, assess initially with MARCH/ABCD approach.
Recognise and treat reversible causes.
Record and correct SpO2 if < 94%, respiratory rate, heart rate, CRT, cardiac monitoring, BP (if possible) and AVPU score.
Establish IV access.
Signs of decompensation include:
Reduced consciousness
Tachypnoea
BP < 5th centile*
CRT > 2 seconds
Weak or impalpable peripheral pulses
Ensure optimal oxygenation with positive pressure ventilation if required.
If unconscious and HR < 60 beats per minute despite oxygenation, start chest compressions.
*Systolic BP 5th Centile (mmHg)
1 month = 50mmHg
1 year = 70mmHg
5 years = 75mmHg
10 years = 80mmHg
If vagal stimulation is a possible cause:
Atropine
Up to 11 years: 20 micrograms/kg IV
12-17 years: 300 – 600 micrograms IV. Larger doses may be used in emergency.
If no response to oxygenation or atropine consider:
Adrenaline
10 micrograms/kg, repeat if necessary
Pacing is rarely required and guided by aetiology.
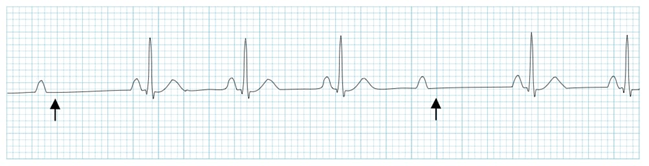
Mobitz Type II Block
Type of second-degree AV node block with intermittent non-conducted P waves without progression of the PR interval. There is a constant PR interval in the conducted beats but some of the P waves are not followed by QRS complexes.
At risk of deteriorating into severe bradycardia, haemodynamic compromise, complete heart block or asystole.
Mobitz Type 2: Arrows indicate 'dropped' QRS complexes or non-conducted p-waves
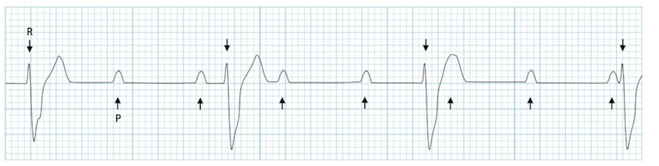
Complete Heart Block
Complete heart block (CHB) occurs when there is total failure of conduction of electrical activity from atria to ventricles and will require cardiac pacing.
CHB is a broad complex bradycardia with no relationship between P waves and QRS complexes. This AV dissociation leads to independent atrial and ventricular rates.